You might also like
- Ab Si Acnee VulgaraDocument9 pagesAb Si Acnee Vulgaraapotek padasukaNo ratings yet
- Dur Sun 2019Document4 pagesDur Sun 2019Dayane GonçalvesNo ratings yet
- Retinoids' effects on vision qualityDocument8 pagesRetinoids' effects on vision qualityUlul AzmiNo ratings yet
- Jurnal Acne 2Document11 pagesJurnal Acne 2Sa'adahNo ratings yet
- MoleculesDocument13 pagesMoleculesMuhammad Ali SyedNo ratings yet
- Acne Treatments: Future Trajectories: Review ArticleDocument7 pagesAcne Treatments: Future Trajectories: Review ArticleIsabel Zamora AuzaNo ratings yet
- DTH 13548Document7 pagesDTH 13548Bryan NguyenNo ratings yet
- Importance of Early Diagnosis and Treatment of AcneDocument7 pagesImportance of Early Diagnosis and Treatment of AcneDimas PrajagoptaNo ratings yet
- Current Issues in The Treatment of Acne VulgarisDocument8 pagesCurrent Issues in The Treatment of Acne VulgarisajiNo ratings yet
- Pharmacotherapy Handbook 9th Edition 2015-BAB KULITDocument19 pagesPharmacotherapy Handbook 9th Edition 2015-BAB KULITCrista Resti StarillaNo ratings yet
- Acne Vulgaris Management: What's New and What's Still True?: Review ArticleDocument5 pagesAcne Vulgaris Management: What's New and What's Still True?: Review ArticleAlmuizzu NurjannahNo ratings yet
- Efinaconazole solution effective topical onychomycosis treatmentDocument9 pagesEfinaconazole solution effective topical onychomycosis treatmentNadia Vinka LisdiantiNo ratings yet
- Terapi Akne Ciproterone Acetate Oleh Dr. Abraham Arimuko SPKK Mars Finsdv FaadvDocument32 pagesTerapi Akne Ciproterone Acetate Oleh Dr. Abraham Arimuko SPKK Mars Finsdv FaadvshabrinaerinNo ratings yet
- 75-Article Text-350-1-10-20220819Document6 pages75-Article Text-350-1-10-20220819Andrianto WongkarNo ratings yet
- Oral Antibiotic Treatment Options For Acne Vulgaris: ReviewDocument7 pagesOral Antibiotic Treatment Options For Acne Vulgaris: ReviewvaiyenNo ratings yet
- Antibiotics Use in DentistryDocument5 pagesAntibiotics Use in DentistryIyad Abou-RabiiNo ratings yet
- Journal DermatologyDocument4 pagesJournal DermatologyKoas PatoNo ratings yet
- 0501 Skin CareDocument9 pages0501 Skin CarekinayungNo ratings yet
- KASUS 1 2nov2010Document5 pagesKASUS 1 2nov2010ninanurfitri2830No ratings yet
- Acne TreatmentDocument2 pagesAcne TreatmentBps Azizah CangkringanNo ratings yet
- Kuliah Akne Vulgaris Sedang BeratDocument41 pagesKuliah Akne Vulgaris Sedang BeratHeny KsNo ratings yet
- JAK Inhibitor Baricitinib in The Treatment of Oral Lichen Planus A Case ReportDocument4 pagesJAK Inhibitor Baricitinib in The Treatment of Oral Lichen Planus A Case ReportAthenaeum Scientific PublishersNo ratings yet
- Chemical Periodontal TherapyDocument23 pagesChemical Periodontal Therapyneji_murniNo ratings yet
- Rhinitis Guidelines: Classification and Differential DiagnosisDocument5 pagesRhinitis Guidelines: Classification and Differential DiagnosisEricaNo ratings yet
- Diagnosis and Treatment of AcneDocument8 pagesDiagnosis and Treatment of AcneFreddy PanjaitanNo ratings yet
- Antibacterial Chemotherapy-Theory, Problems, and Practice (Oxford University Press)Document93 pagesAntibacterial Chemotherapy-Theory, Problems, and Practice (Oxford University Press)francieudo1No ratings yet
- G AntibioticTherapyDocument3 pagesG AntibioticTherapyJacoboGonzálezNo ratings yet
- FTX Infeksi JamurDocument64 pagesFTX Infeksi JamurNafisah SofiaNo ratings yet
- Lichen Planus PDFDocument5 pagesLichen Planus PDFRobins DhakalNo ratings yet
- SDVKN IonqioDocument5 pagesSDVKN IonqiodzivahNo ratings yet
- Tinea CorporisDocument7 pagesTinea CorporisAziza Ulfie WijayaniNo ratings yet
- Diagnosis and Treatment of Acne: A Guide for Primary CareDocument17 pagesDiagnosis and Treatment of Acne: A Guide for Primary CareluthfiNo ratings yet
- Antiemetic Drug Use in Children What The.3Document6 pagesAntiemetic Drug Use in Children What The.3Zafitri AsrulNo ratings yet
- Terbinafine: A Position Statement of The NSW Therapeutic Assessment Group IncDocument17 pagesTerbinafine: A Position Statement of The NSW Therapeutic Assessment Group Incedy744No ratings yet
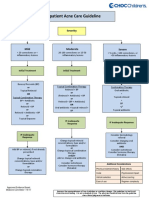
- Outpatient Acne Care Guideline: SeverityDocument5 pagesOutpatient Acne Care Guideline: SeverityMarrauNo ratings yet
- Gupta2014Document7 pagesGupta2014Lodewyk Kefas JoshoaNo ratings yet
- Treatment of Scabies: Comparative Study of EfficacyDocument7 pagesTreatment of Scabies: Comparative Study of EfficacyLamtioma GultomNo ratings yet
- BP AntibiotictherapyDocument4 pagesBP AntibiotictherapyDebasmita Datta GuptaNo ratings yet
- Tinea CorporisDocument7 pagesTinea CorporisAziza Ulfie WijayaniNo ratings yet
- Intra Canal Medicaments-2Document58 pagesIntra Canal Medicaments-2FadilaNo ratings yet
- 04 - 01 - Sarra Mutiara Adev - Artikel Jurnal Dan Resume Artikel JurnalDocument23 pages04 - 01 - Sarra Mutiara Adev - Artikel Jurnal Dan Resume Artikel Jurnalsarra mutiara adevNo ratings yet
- Hydrocortisone With Ethanol in ADDocument6 pagesHydrocortisone With Ethanol in ADAlikaa RizkiiNo ratings yet
- Topical Retinoids in Acne Vulgaris: A Systematic ReviewDocument21 pagesTopical Retinoids in Acne Vulgaris: A Systematic ReviewFitri Aesthetic centerNo ratings yet
- DR Meera Kuppusamy MBBS (IMU), MRCP (UK), Adv Derm Masters (UKM) Consultant Dermatologist Columbia Asia KlangDocument86 pagesDR Meera Kuppusamy MBBS (IMU), MRCP (UK), Adv Derm Masters (UKM) Consultant Dermatologist Columbia Asia KlangdnaielNo ratings yet
- Hormonas and AcneDocument3 pagesHormonas and AcneRistiana Suci d'KemponNo ratings yet
- Use of Antibiotic Therapy For Pediatric Dental Patients: Latest RevisionDocument4 pagesUse of Antibiotic Therapy For Pediatric Dental Patients: Latest Revisionnona aryanNo ratings yet
- Acne and Niacinamide 2017 dth.12481Document7 pagesAcne and Niacinamide 2017 dth.12481Vita BūdvytėNo ratings yet
- Management of Oral Lichen Planus: Review ArticleDocument5 pagesManagement of Oral Lichen Planus: Review ArticlebunapiNo ratings yet
- Adverse Drug Reaction JalpaDocument7 pagesAdverse Drug Reaction Jalpaparmar jalpabenNo ratings yet
- JournalDocument12 pagesJournaltamiNo ratings yet
- Efficacy of Terbinafne vs Eberconazole Creams for TineaDocument4 pagesEfficacy of Terbinafne vs Eberconazole Creams for TineaBayu Zeva WirasaktiNo ratings yet
- Local Antimicrobial TherapyDocument87 pagesLocal Antimicrobial TherapyDrAbhishek SinhaNo ratings yet
- IMW025.04 Immunoglobulin Handbood Diphtheria Update AUG 2018 v2Document9 pagesIMW025.04 Immunoglobulin Handbood Diphtheria Update AUG 2018 v2Ak62442No ratings yet
- Evidence For The Effi Cacy of Over-The-Counter Vitamin A Cosmetic Products in The Improvement of Facial Skin AgingDocument8 pagesEvidence For The Effi Cacy of Over-The-Counter Vitamin A Cosmetic Products in The Improvement of Facial Skin AgingCuiting FengNo ratings yet
- Pharmacology MCQsDocument88 pagesPharmacology MCQsDr.Tawheed86% (7)
- Oral Health Complications and HIV-Infected PatientsDocument14 pagesOral Health Complications and HIV-Infected PatientsTemesgen EndalewNo ratings yet
- McfaldaDocument3 pagesMcfaldaMario RodriguezySilvaNo ratings yet
- Pharmacology in EndodonticsDocument7 pagesPharmacology in EndodonticsJanice EstaNo ratings yet
- Non Antibiotic AcneDocument34 pagesNon Antibiotic AcneAdrian SyahNo ratings yet
- SialolithiasisDocument15 pagesSialolithiasisHemant BaonerkarNo ratings yet
- Prion Disease: Kelly J. Baldwin, MD Cynthia M. Correll, MDDocument12 pagesPrion Disease: Kelly J. Baldwin, MD Cynthia M. Correll, MDMerari Lugo Ocaña100% (1)
- Acute Kidney Injury in Pediatrics: An Overview Focusing On PathophysiologyDocument16 pagesAcute Kidney Injury in Pediatrics: An Overview Focusing On PathophysiologyDr.gendjutNo ratings yet
- 9.cancer of The Female Genital Tract.Document58 pages9.cancer of The Female Genital Tract.vichramNo ratings yet
- Litchi, The Unlucky Fruit What Does The Evidence SayDocument18 pagesLitchi, The Unlucky Fruit What Does The Evidence SaySaujanyaNo ratings yet
- Training Needs Assessment of Poultry Farmers in TeDocument4 pagesTraining Needs Assessment of Poultry Farmers in TeGia MNo ratings yet
- Morning Report Pediatric DepartmentDocument18 pagesMorning Report Pediatric DepartmentMedina MarwanNo ratings yet
- Designing Classrooms for Students with Intellectual DisabilitiesDocument31 pagesDesigning Classrooms for Students with Intellectual DisabilitiesVyshnav PvNo ratings yet
- 4thamended ComplaintDocument25 pages4thamended Complaintapi-521619243No ratings yet
- 2.1 Medical Surgical Nursing - I Papers QPDocument15 pages2.1 Medical Surgical Nursing - I Papers QPAnju KarunakaranNo ratings yet
- Ypgh 113 1695081Document12 pagesYpgh 113 1695081Pawan MishraNo ratings yet
- NDT Session 8 (The Vitamins)Document6 pagesNDT Session 8 (The Vitamins)Julia Rae Delos SantosNo ratings yet
- Life Skills 3 and 4-1Document55 pagesLife Skills 3 and 4-1Wakale Nzako100% (1)
- Clinical Management of Injured Birds-of-PreyDocument9 pagesClinical Management of Injured Birds-of-PreyLjón BjörnNo ratings yet
- The University of Jordan/ Faculty of Graduate Studies. Faculty of Medicine Family and Community Medicine DepartmentDocument39 pagesThe University of Jordan/ Faculty of Graduate Studies. Faculty of Medicine Family and Community Medicine DepartmentOhood ShunnarNo ratings yet
- Adjuvant Therapy With Serratiopeptidase and Vitamin D For COVID-19 Patients: A New PerspectiveDocument7 pagesAdjuvant Therapy With Serratiopeptidase and Vitamin D For COVID-19 Patients: A New PerspectiveKaterina PoposkaNo ratings yet
- StrokeDocument17 pagesStrokeRama KrishnaNo ratings yet
- Case StudyDocument2 pagesCase StudyClaire MachicaNo ratings yet
- Diagnostic Accuracy of F-Methylcholine Positron Emission Tomography/Computed Tomography For Intra-And Extrahepatic Hepatocellular CarcinomaDocument11 pagesDiagnostic Accuracy of F-Methylcholine Positron Emission Tomography/Computed Tomography For Intra-And Extrahepatic Hepatocellular CarcinomaRais KhairuddinNo ratings yet
- Mother Tinctures in HomoeopathyDocument9 pagesMother Tinctures in HomoeopathyRaghu ThotaNo ratings yet
- Drug Study - Cefixime PDFDocument1 pageDrug Study - Cefixime PDF2C- VILLACARLOS, LEONA ROSE M.No ratings yet
- ENT Prelims TransDocument45 pagesENT Prelims TransRaven CocjinNo ratings yet
- Stanley T. Agor, MD, DPPS, MSPH Department of Pediatrics Cagayan Valley Medical CenterDocument35 pagesStanley T. Agor, MD, DPPS, MSPH Department of Pediatrics Cagayan Valley Medical CenterLuis PadillaNo ratings yet
- Fill in The Blanks Using "Should" or Shouldn't and A Suitable Verb From The List ProvidedDocument1 pageFill in The Blanks Using "Should" or Shouldn't and A Suitable Verb From The List ProvidedDragana ZafirovskaNo ratings yet
- Parkinson DiseaseDocument11 pagesParkinson Diseaseapi-508611307No ratings yet
- Pulmonology 3 COPD (Completed)Document6 pagesPulmonology 3 COPD (Completed)Benjamin NgNo ratings yet
- OsteoporoseDocument54 pagesOsteoporoseJandui DinizNo ratings yet
- Effects: PharmacokineticsDocument7 pagesEffects: PharmacokineticsShiraz SiddiquiNo ratings yet
- DrowningDocument9 pagesDrowningCarlos Alberto Torres LópezNo ratings yet
- CASE REPORT PsychiatryDocument6 pagesCASE REPORT PsychiatryTJ LoNo ratings yet