You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Cardiovascular DiseasesDocument8 pagesCardiovascular DiseasesRebecca MarshallNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Antihypertensives Drug ChartDocument3 pagesAntihypertensives Drug Chartinfirmarydude100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 4-Cylinder Direct Injection Engine (1 8 2 0 LTR 4-Valve TFSI - Generation III)Document315 pages4-Cylinder Direct Injection Engine (1 8 2 0 LTR 4-Valve TFSI - Generation III)Martin huntNo ratings yet
- 03 Pharmacotherapy Vol 2 Cardiology IIDocument68 pages03 Pharmacotherapy Vol 2 Cardiology IIعلى الجارحىNo ratings yet
- Topic 2 - Adrenergic DrugsDocument52 pagesTopic 2 - Adrenergic DrugsAngeli Gregorio100% (1)
- Bonaire Multi Appliance Comfort ControlDocument52 pagesBonaire Multi Appliance Comfort ControlMartin huntNo ratings yet
- 4-Cylinder TDI Engine 2 0 LTR 4-Valve Common Rail (EA 288 Gen I)Document364 pages4-Cylinder TDI Engine 2 0 LTR 4-Valve Common Rail (EA 288 Gen I)Martin hunt0% (1)
- Bisoprolol in HypertensionDocument35 pagesBisoprolol in HypertensionjimNo ratings yet
- 715 PrometricDocument61 pages715 PrometricNosheen HaqNo ratings yet
- Drug Study - ErcefloraDocument4 pagesDrug Study - ErcefloraKrisia Castuciano50% (2)
- FANUC Series 0-PC Function Connection Manual B-64153EN01 CNC ManualDocument148 pagesFANUC Series 0-PC Function Connection Manual B-64153EN01 CNC ManualMartin huntNo ratings yet
- Fanuc Controller Fanuc Controller Mechanical Fanuc Controller Mechanical LubricationDocument2 pagesFanuc Controller Fanuc Controller Mechanical Fanuc Controller Mechanical LubricationMartin huntNo ratings yet
- Medical Masterclass 2-Scientific Background To Medicine 2 PDFDocument136 pagesMedical Masterclass 2-Scientific Background To Medicine 2 PDFAnonymous oQtve4oNo ratings yet
- Clinical Pharmacology Book 2018Document304 pagesClinical Pharmacology Book 2018Sumaiya Islam KhanNo ratings yet
- HAAD Exam 06-08-2020Document16 pagesHAAD Exam 06-08-2020Sandeep Kanneganti100% (2)
- Vbe 1500Document16 pagesVbe 1500Martin huntNo ratings yet
- Cannabis Legalisation Bill 2022.unDocument30 pagesCannabis Legalisation Bill 2022.unMartin huntNo ratings yet
- Endorsed Community Safety Strategy October 2019Document23 pagesEndorsed Community Safety Strategy October 2019Martin huntNo ratings yet
- GWM Ute Cannon Service ScheduleDocument1 pageGWM Ute Cannon Service ScheduleMartin huntNo ratings yet
- Mill Quad FeedDocument12 pagesMill Quad FeedMartin huntNo ratings yet
- Bonaire Evaporative Touch Pad ControlDocument32 pagesBonaire Evaporative Touch Pad ControlMartin huntNo ratings yet
- Service: ManualDocument82 pagesService: ManualMartin huntNo ratings yet
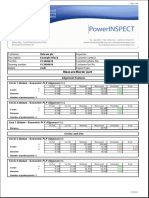
- Meas Ure:mas Ter PartDocument6 pagesMeas Ure:mas Ter PartMartin huntNo ratings yet
- FANUC FL-Net Board Operators Manual GFZ-63434EN02 CNC ManualDocument138 pagesFANUC FL-Net Board Operators Manual GFZ-63434EN02 CNC ManualMartin huntNo ratings yet
- Pne2002 Series ControlDocument16 pagesPne2002 Series ControlMartin huntNo ratings yet
- Sinus TachycardiaDocument87 pagesSinus TachycardiaMartin huntNo ratings yet
- Zte Blade A3: Downloaded From Manuals Search EngineDocument67 pagesZte Blade A3: Downloaded From Manuals Search EngineMartin huntNo ratings yet
- Bonaire Commercial B SeriesDocument28 pagesBonaire Commercial B SeriesMartin huntNo ratings yet
- Kathy - Inappropriate Sinus Tachycardia (IST)Document4 pagesKathy - Inappropriate Sinus Tachycardia (IST)Martin huntNo ratings yet
- Painting Swimming Pools: UnpaintedDocument2 pagesPainting Swimming Pools: UnpaintedMartin huntNo ratings yet
- Recoating Swimming Pools: Maintenance ChallengesDocument3 pagesRecoating Swimming Pools: Maintenance ChallengesMartin huntNo ratings yet
- Rigging Manual V2Document63 pagesRigging Manual V2Martin huntNo ratings yet
- Administering Metoprolol IV Push 1Document22 pagesAdministering Metoprolol IV Push 1api-357388170No ratings yet
- Guias Hipertension 2023 Esc DDocument11 pagesGuias Hipertension 2023 Esc Dmiguel contrerasNo ratings yet
- Applied Therapeutic I: Case StudyDocument15 pagesApplied Therapeutic I: Case StudyJean LaiNo ratings yet
- Chapter 1 - Pharmacotherapy of The Ophthalmic - 2008 - Clinical Ocular PharmacoDocument13 pagesChapter 1 - Pharmacotherapy of The Ophthalmic - 2008 - Clinical Ocular PharmacosNo ratings yet
- Hemodynamic response to β-blockers in severe sepsis and septic shock: A review of current literatureDocument6 pagesHemodynamic response to β-blockers in severe sepsis and septic shock: A review of current literatureIris AszalosNo ratings yet
- Drugs Acting On The Autonomic Nervous SystemDocument68 pagesDrugs Acting On The Autonomic Nervous SystemjisooNo ratings yet
- Sympathomimetics Drugs REVIEWDocument9 pagesSympathomimetics Drugs REVIEWLyca SalardaNo ratings yet
- Notes On anti-HTN Drugs (Public Edition)Document17 pagesNotes On anti-HTN Drugs (Public Edition)Abdullah Al ArifNo ratings yet
- Kasus 3 KardiovaskularDocument3 pagesKasus 3 KardiovaskularHelmin DhNo ratings yet
- Acute Exacerbation of Congestive Heart Failure: History & ExamDocument76 pagesAcute Exacerbation of Congestive Heart Failure: History & ExamMicija CucuNo ratings yet
- 13 Antihypertensive Drugs (Notes - Q A) AtfDocument3 pages13 Antihypertensive Drugs (Notes - Q A) AtfFeven AbrahamNo ratings yet
- Case Presentation On Systemic Lupus Erythematosus (SLE) : Presented By: Mahitha Karimsetti 616175802018 Pharm. D InternDocument35 pagesCase Presentation On Systemic Lupus Erythematosus (SLE) : Presented By: Mahitha Karimsetti 616175802018 Pharm. D Internsrija vijjapuNo ratings yet
- Adrenergic AntagonistsDocument18 pagesAdrenergic AntagonistsKarina MadriagaNo ratings yet
- PMN 310 Anti-Anginal Drugs: by Manasseh Mvula Bsc. N Iii StudentDocument54 pagesPMN 310 Anti-Anginal Drugs: by Manasseh Mvula Bsc. N Iii StudentManasseh MvulaNo ratings yet
- Optimal Local Anaesthesia For Dentistry: Tara RentonDocument11 pagesOptimal Local Anaesthesia For Dentistry: Tara RentonbabukanchaNo ratings yet
- Drugs Used in Cardiovascular SystemDocument57 pagesDrugs Used in Cardiovascular SystemSandeep ChaudharyNo ratings yet
- Decompensated Congestive Cardiac Failure Secondary To No1Document4 pagesDecompensated Congestive Cardiac Failure Secondary To No1Qi YingNo ratings yet
- Cardiovascular Pharmacology: Ana Sharmaine S. Uera, MD DR PJGMRMC Anesthesiology Department 1st Year ResidentDocument68 pagesCardiovascular Pharmacology: Ana Sharmaine S. Uera, MD DR PJGMRMC Anesthesiology Department 1st Year ResidentLalay CabanagNo ratings yet
- Chapter ReviewDocument32 pagesChapter ReviewThanh TrúcNo ratings yet
- Definition: The Ability To Use Strength Quickly To Produce An Explosive EffortDocument41 pagesDefinition: The Ability To Use Strength Quickly To Produce An Explosive Effortdeepa sharmaNo ratings yet