You might also like
- A Guide To Psychotropic DrugsDocument16 pagesA Guide To Psychotropic DrugsNokz M. Raki-inNo ratings yet
- Types and Uses of Anti-Anxiety DrugsDocument39 pagesTypes and Uses of Anti-Anxiety DrugsArkene LevyNo ratings yet
- Training Needs AssessmentDocument11 pagesTraining Needs AssessmentKarina Madriaga100% (1)
- 1013 Vasoactive Agents in ShockDocument20 pages1013 Vasoactive Agents in Shockrogelio cruzNo ratings yet
- Antiepileptic Drugs and Parkinson's Disease PharmacologyDocument50 pagesAntiepileptic Drugs and Parkinson's Disease PharmacologymayraNo ratings yet
- Intensive Care Unit (ICU) Manual 2020-21Document146 pagesIntensive Care Unit (ICU) Manual 2020-21anithaNo ratings yet
- Understanding Cardiomyopathies and Cardiac Conduction DisordersDocument86 pagesUnderstanding Cardiomyopathies and Cardiac Conduction DisordersStarr Newman100% (1)
- PharmacologyDocument236 pagesPharmacologyyalahopa100% (2)
- Antihypertensives Summary Katzung PharmacologyDocument8 pagesAntihypertensives Summary Katzung PharmacologyRobin TolentinoNo ratings yet
- Fall PreventionDocument108 pagesFall Preventionsubinj_3No ratings yet
- Complication of Hemodialysis and Their ManagementDocument52 pagesComplication of Hemodialysis and Their ManagementRetno SumaraNo ratings yet
- 41 - Type of Shock PDFDocument2 pages41 - Type of Shock PDFjamesNo ratings yet
- Guideline HypoglycemiaDocument6 pagesGuideline HypoglycemialeslyjanetNo ratings yet
- Complications of Spinal and Epidural AnesthesiaDocument45 pagesComplications of Spinal and Epidural AnesthesiashikhaNo ratings yet
- Causes, Symptoms and Treatment of Low Blood Pressure (HypotensionDocument4 pagesCauses, Symptoms and Treatment of Low Blood Pressure (Hypotensionclubsanatate100% (1)
- Antiadrenergic DrugsDocument44 pagesAntiadrenergic DrugsHUZAIFA YAMAANNo ratings yet
- PharmTest3 StudyGuideDocument9 pagesPharmTest3 StudyGuideTara Bickford ManisNo ratings yet
- Anemia in PregnancyDocument9 pagesAnemia in PregnancyKarina Madriaga100% (2)
- Infections During PregnancyDocument9 pagesInfections During PregnancyKarina Madriaga100% (4)
- Adrenergic Antagonists: An Introduction to Alpha and Beta BlockersDocument64 pagesAdrenergic Antagonists: An Introduction to Alpha and Beta BlockersAneeza AhmadNo ratings yet
- Fundamentals of Nursing (Midterm Topic 2)Document7 pagesFundamentals of Nursing (Midterm Topic 2)Manuel, Precious Marie B.No ratings yet
- Soal Post TestDocument70 pagesSoal Post Testananda96% (25)
- Family Nursing Care PlanDocument3 pagesFamily Nursing Care PlanAlexa Abidin Oldenborg96% (28)
- Drug Dosage, Classification, Indications, and Nursing ResponsibilitiesDocument12 pagesDrug Dosage, Classification, Indications, and Nursing ResponsibilitiesCamilley De Vera100% (1)
- 5 SympatholyticsDocument27 pages5 SympatholyticsHussain RazaNo ratings yet
- Antagonis AdrenergikDocument34 pagesAntagonis AdrenergikGde Ananda ArmanditaNo ratings yet
- Adrenergic AntagonistsDocument10 pagesAdrenergic AntagonistsArjay LucenaNo ratings yet
- Drugs Acting On The Autonomic Nervous SystemDocument12 pagesDrugs Acting On The Autonomic Nervous SystemAj GoNo ratings yet
- Adrenergic AgonistsDocument18 pagesAdrenergic AgonistsJod Bell100% (1)
- Alpha BlockersDocument21 pagesAlpha BlockersMaricris PallarNo ratings yet
- Adrenergic AntagonistsDocument44 pagesAdrenergic AntagonistsTsegaye HailuNo ratings yet
- 7,8 - Antihypertensive DrugsDocument10 pages7,8 - Antihypertensive DrugsHusniya MehamedNo ratings yet
- Fight-or-Flight Response and Rest-and-Digest via ANSDocument5 pagesFight-or-Flight Response and Rest-and-Digest via ANSCadorna Chesca LoboNo ratings yet
- Adrenergic Antagonists Adrenoreceptor Blockers 2: September 2019Document30 pagesAdrenergic Antagonists Adrenoreceptor Blockers 2: September 2019Rohullah QasimiNo ratings yet
- 5 Adrenoceptor BlockersDocument52 pages5 Adrenoceptor BlockersHamid Hussain HamidNo ratings yet
- Alpha Blockers PharmacologyDocument23 pagesAlpha Blockers PharmacologyHesbon MomanyiNo ratings yet
- Adrenergic Drugs: ''Sympathomimetics & Sympatholytics"Document17 pagesAdrenergic Drugs: ''Sympathomimetics & Sympatholytics"SimonNo ratings yet
- 41.antihypertensive DrugsDocument75 pages41.antihypertensive DrugspradeephdNo ratings yet
- SY - Medichem i - adrenergic blockers (1)Document38 pagesSY - Medichem i - adrenergic blockers (1)KevalNo ratings yet
- Adrenergic AntagonistsDocument29 pagesAdrenergic AntagonistsBenedict Brashi100% (1)
- SympatholyticsDocument46 pagesSympatholyticsHari Kamesh KiranNo ratings yet
- L20 - Adrenergic VDocument10 pagesL20 - Adrenergic Vyasaira707No ratings yet
- 6 SymaptholyticDocument48 pages6 SymaptholyticYoueel IbrahemNo ratings yet
- Adrenoreceptor Antagonist: Leida Marie P. Alarcon, MD, FPAFPDocument23 pagesAdrenoreceptor Antagonist: Leida Marie P. Alarcon, MD, FPAFPKenneth NuñezNo ratings yet
- OBAT ANTIHIPERTENSI YANG EFEKTIFDocument38 pagesOBAT ANTIHIPERTENSI YANG EFEKTIFNi Made Dwiki AndriyaniNo ratings yet
- Antiadrenergic 180630054321Document19 pagesAntiadrenergic 180630054321Dinam Gyatso AadHenmooNo ratings yet
- CH 19Document15 pagesCH 19Emmanuel GaliciaNo ratings yet
- Alpha 1 Blocker: Obstruction and Relieving Effects of Benign Prostatic Hyperplasia BPHDocument21 pagesAlpha 1 Blocker: Obstruction and Relieving Effects of Benign Prostatic Hyperplasia BPHKaylee LengNo ratings yet
- Adrenergic Antagonist (2013)Document23 pagesAdrenergic Antagonist (2013)Akmal SafwanNo ratings yet
- Chapter 31: Adrenergic Antagonists: Drug ListDocument7 pagesChapter 31: Adrenergic Antagonists: Drug ListMariah Jane TaladuaNo ratings yet
- Adrenargic Antiagonist Prepardd by BashirDocument11 pagesAdrenargic Antiagonist Prepardd by BashirZakarie Abdullahi HusseinNo ratings yet
- Drugsssss For ScrapDocument17 pagesDrugsssss For ScrapCAMILLE GAIL HADJIRANINo ratings yet
- Adrenergic Drugs 2015Document48 pagesAdrenergic Drugs 2015Rizki SariWahyuniNo ratings yet
- Antianginal Drugs Antianginal Drugs Are Used Primarily To Restore The Balance Between TheDocument10 pagesAntianginal Drugs Antianginal Drugs Are Used Primarily To Restore The Balance Between TheMIR SARTAJNo ratings yet
- Sympa T Holy TicsDocument30 pagesSympa T Holy TicsAhaisibwe GordonNo ratings yet
- Adrenoceptor Antagonists Classification & Clinical UsesDocument23 pagesAdrenoceptor Antagonists Classification & Clinical UsesMirza Shaharyar BaigNo ratings yet
- ANAESTHETICSDocument16 pagesANAESTHETICSAmbroseNo ratings yet
- ReghDocument9 pagesReghreghpineda28No ratings yet
- Adrenergic Drugs Affecting the Autonomic Nervous SystemDocument11 pagesAdrenergic Drugs Affecting the Autonomic Nervous SystemchareneadamsNo ratings yet
- Drug StudyDocument4 pagesDrug StudyEmilyne Joy Mendoza CabayaNo ratings yet
- Hypertension: Increase in Blood PressureDocument29 pagesHypertension: Increase in Blood PressureKeesha Mae AnteNo ratings yet
- Extrapyramidal SymptomsDocument5 pagesExtrapyramidal SymptomsGenette Sy SolisNo ratings yet
- Medications For The ElderlyDocument8 pagesMedications For The ElderlyShawn TaylorNo ratings yet
- Adrenergic Antagonists (Sympatholytics)Document27 pagesAdrenergic Antagonists (Sympatholytics)Huzaifa KhaleeqNo ratings yet
- Prototype Drug - Adrenergic AgonistDocument1 pagePrototype Drug - Adrenergic Agonistshiloh Paradis100% (1)
- Kimia Medisinal Antiadrenergic 4BDocument46 pagesKimia Medisinal Antiadrenergic 4BDina Sulastiyo MurtiNo ratings yet
- Neuropharmacology Agents in Neuroscience NursingDocument36 pagesNeuropharmacology Agents in Neuroscience NursingDebika DasNo ratings yet
- Opiate Analgesics and Clinical UsesDocument40 pagesOpiate Analgesics and Clinical UsesAnonymous 7hJgATNo ratings yet
- Adrenoceptor Blocking Drugs: Department of Pharmacology College of Medicine-University of Kirkuk 2019-2020Document44 pagesAdrenoceptor Blocking Drugs: Department of Pharmacology College of Medicine-University of Kirkuk 2019-2020OMAR NASSERNo ratings yet
- Nursing Sympathomimetics and SympatholyticsDocument87 pagesNursing Sympathomimetics and SympatholyticsFrancis PeterosNo ratings yet
- Antianginal Drugs Are Used Primarily To Restore The Balance Between The Oxygen SupplyDocument8 pagesAntianginal Drugs Are Used Primarily To Restore The Balance Between The Oxygen SupplyUzma KhanNo ratings yet
- Bimbel Ukmppd FarmakoDocument92 pagesBimbel Ukmppd FarmakoJavier AntaresNo ratings yet
- Adrenolytics Jurusan Pendidikan Dokter Umum Fakultas Kedokteran Universitas SriwijayaDocument33 pagesAdrenolytics Jurusan Pendidikan Dokter Umum Fakultas Kedokteran Universitas SriwijayaagungNo ratings yet
- Alpha - Beta Adrenergic BlockersDocument7 pagesAlpha - Beta Adrenergic BlockersAli RizgarNo ratings yet
- Adrenergic Antagonist PharmacologyDocument60 pagesAdrenergic Antagonist PharmacologyJohn Benedict VocalesNo ratings yet
- Activity 5 Community Health Care ProcessDocument16 pagesActivity 5 Community Health Care ProcessKarina MadriagaNo ratings yet
- Risk For Decreased Cardiac Tissue PerfusionDocument3 pagesRisk For Decreased Cardiac Tissue PerfusionKarina MadriagaNo ratings yet
- Drug StudyDocument60 pagesDrug StudyKarina MadriagaNo ratings yet
- Goal Met.: Polymorphonuclea R LeukocytesDocument2 pagesGoal Met.: Polymorphonuclea R LeukocytesKarina MadriagaNo ratings yet
- Activity 4Document1 pageActivity 4Karina MadriagaNo ratings yet
- NCM 113 - Timeline of TopicsDocument8 pagesNCM 113 - Timeline of TopicsKarina MadriagaNo ratings yet
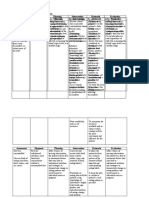
- NCPsDocument3 pagesNCPsKarina MadriagaNo ratings yet
- Mucocutaneous Lymph Node SyndromeDocument9 pagesMucocutaneous Lymph Node SyndromeKarina MadriagaNo ratings yet
- Midterms Group 5Document25 pagesMidterms Group 5Karina MadriagaNo ratings yet
- FreedomDocument1 pageFreedomKarina MadriagaNo ratings yet
- Mucocutaneous Lymph Node SyndromeDocument9 pagesMucocutaneous Lymph Node SyndromeKarina MadriagaNo ratings yet
- Beatitudes Beatitudes As Enshrined in The Filipino Character Reversal of The Beatitudes/ DisvaluesDocument2 pagesBeatitudes Beatitudes As Enshrined in The Filipino Character Reversal of The Beatitudes/ DisvaluesKarina MadriagaNo ratings yet
- JusticeDocument3 pagesJusticeKarina MadriagaNo ratings yet
- HUMAN AS MORAL AGENTDocument2 pagesHUMAN AS MORAL AGENTKarina MadriagaNo ratings yet
- The Eight Beatitudes of JesusDocument2 pagesThe Eight Beatitudes of JesusKarina MadriagaNo ratings yet
- NonmaleficenceDocument3 pagesNonmaleficenceKarina MadriagaNo ratings yet
- Assignment For BSN 3 - A - RLEDocument2 pagesAssignment For BSN 3 - A - RLEKarina Madriaga100% (1)
- Community Organizing Participatory Action ResearchDocument8 pagesCommunity Organizing Participatory Action ResearchKarina MadriagaNo ratings yet
- Nutrition and Bone Health: Group 6Document22 pagesNutrition and Bone Health: Group 6Karina MadriagaNo ratings yet
- GEC 109 August 15Document1 pageGEC 109 August 15Karina MadriagaNo ratings yet
- Lesson 2Document6 pagesLesson 2Karina MadriagaNo ratings yet
- Prenatal Care Common Discomforts During PregnancyDocument5 pagesPrenatal Care Common Discomforts During PregnancyKarina MadriagaNo ratings yet
- August 14Document2 pagesAugust 14Karina MadriagaNo ratings yet
- Official View Similarities Popular ViewDocument1 pageOfficial View Similarities Popular ViewKarina MadriagaNo ratings yet
- Official View Similarities Popular ViewDocument1 pageOfficial View Similarities Popular ViewKarina MadriagaNo ratings yet
- Lesson-1 3Document14 pagesLesson-1 3Karina MadriagaNo ratings yet
- Nursing Care Plan: Group 4-Open Wound Head Injury After Debris FallDocument3 pagesNursing Care Plan: Group 4-Open Wound Head Injury After Debris FallNicole Villanueva, BSN - Level 3ANo ratings yet
- Body Temperature-1Document5 pagesBody Temperature-1سماح صلاحNo ratings yet
- Acute Traumatic Spinal Cord InjuryDocument18 pagesAcute Traumatic Spinal Cord InjurymedilearnersNo ratings yet
- Musculoskeletal SystemDocument60 pagesMusculoskeletal Systempetite_chien15No ratings yet
- Critical Care Cardiovascular Disease Chapter 22: Classification, Pathophysiology, and Management of ShockDocument44 pagesCritical Care Cardiovascular Disease Chapter 22: Classification, Pathophysiology, and Management of Shockismi latifahNo ratings yet
- Postpartum Purulent-Septic Diseases (Peritonitis, Sepsis, Toxic-Infectious Shock)Document64 pagesPostpartum Purulent-Septic Diseases (Peritonitis, Sepsis, Toxic-Infectious Shock)Muhammed ElnakibNo ratings yet
- The Effects of Prophylactic Bolus Phenylephrine On Hypotension During Low-Dose Spinal Anesthesia For Cesarean SectionDocument6 pagesThe Effects of Prophylactic Bolus Phenylephrine On Hypotension During Low-Dose Spinal Anesthesia For Cesarean SectionAgus GunardiNo ratings yet
- Seminar - Hemorrhage 25-06-2020Document75 pagesSeminar - Hemorrhage 25-06-2020Chandra dimpleNo ratings yet
- Hemorrhagic Shock - The "Physiology Approach"Document18 pagesHemorrhagic Shock - The "Physiology Approach"carloshgmedeirosNo ratings yet
- Recent Advances in The Management of Hypoxic-Ischemic Encephalopathy-IJPPDocument6 pagesRecent Advances in The Management of Hypoxic-Ischemic Encephalopathy-IJPPdrtgodeNo ratings yet
- DRUG STUDY (Preeclampsia)Document11 pagesDRUG STUDY (Preeclampsia)Jobelle AcenaNo ratings yet
- Drug Data For TomDocument2 pagesDrug Data For TomAbdelmar SusulanNo ratings yet
- Nursing Care Plan for Mrs. ReyesDocument3 pagesNursing Care Plan for Mrs. ReyesElishah CaprichoNo ratings yet
- HaemaccelinfDocument9 pagesHaemaccelinfSisca YulistianaNo ratings yet
- Cardiac Tamponade - Drug StudyDocument4 pagesCardiac Tamponade - Drug StudyktNo ratings yet
- Evaluation of The Relationship Between Peripheral Pulse Palpation and Doppler Systolic Blood Pressure in Dogs Presenting To An Emergency ServiceDocument6 pagesEvaluation of The Relationship Between Peripheral Pulse Palpation and Doppler Systolic Blood Pressure in Dogs Presenting To An Emergency ServiceYissette Bautista CarrilloNo ratings yet
- Auspar Sacubitril Valsartan Salt Complex 160923 PiDocument27 pagesAuspar Sacubitril Valsartan Salt Complex 160923 PiMayson BaliNo ratings yet
- DO NOT Take Telmisartan TabletsDocument6 pagesDO NOT Take Telmisartan Tabletssaurabh_shrutiNo ratings yet