You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Dispossessed of Necropolitics On The San DiegoDocument15 pagesThe Dispossessed of Necropolitics On The San DiegoSilverio CasillasNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- International Journal of Drug PolicyDocument7 pagesInternational Journal of Drug PolicySilverio CasillasNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Interdisciplinary Approaches To The Phenomenology of Auditory Verbal HallucinationsDocument9 pagesInterdisciplinary Approaches To The Phenomenology of Auditory Verbal HallucinationsSilverio CasillasNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Thomas J. Csordas: Culture, Medicine and Psychiatry 28: 1-14, 2004Document14 pagesThomas J. Csordas: Culture, Medicine and Psychiatry 28: 1-14, 2004Silverio CasillasNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Cigarro y MethDocument13 pagesCigarro y MethSilverio CasillasNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- "Somebody Is Gonna Be Hurt": Involuntary Drug Treatment in MexicoDocument16 pages"Somebody Is Gonna Be Hurt": Involuntary Drug Treatment in MexicoSilverio CasillasNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Who Are Deemed The Worthy and Unworthy Victims of Mexico S Drug Related ViolenceDocument16 pagesWho Are Deemed The Worthy and Unworthy Victims of Mexico S Drug Related ViolenceSilverio CasillasNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- General Strain Theory, Depression, and Substance Use: Results From A Nationally Representative, Longitudinal Sample of White, African-American, and Hispanic Adolescents and Young A..Document20 pagesGeneral Strain Theory, Depression, and Substance Use: Results From A Nationally Representative, Longitudinal Sample of White, African-American, and Hispanic Adolescents and Young A..Silverio CasillasNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- PASSOS 2020 BreakingtheLawtoEnsureOrderDocument16 pagesPASSOS 2020 BreakingtheLawtoEnsureOrderSilverio CasillasNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Ni Hms 928844Document17 pagesNi Hms 928844Silverio CasillasNo ratings yet
- The Change of Behavioural Methamphetamine Effect After Repeated MDMA Administration in MiceDocument7 pagesThe Change of Behavioural Methamphetamine Effect After Repeated MDMA Administration in MiceSilverio CasillasNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Use of Clinical Trials in Comparative Effectiv PDFDocument9 pagesThe Use of Clinical Trials in Comparative Effectiv PDFSilverio CasillasNo ratings yet
- The Nurture Versus Biosocial Debate in Criminology: On The Origins of Criminal Behavior and CriminalityDocument20 pagesThe Nurture Versus Biosocial Debate in Criminology: On The Origins of Criminal Behavior and CriminalitySilverio CasillasNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- N & C Explorations: China Isn't A Country It's A Different WorldDocument20 pagesN & C Explorations: China Isn't A Country It's A Different WorldSilverio CasillasNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Gray Hat Hacking The Ethical Hackers Handbook Sixth Edition Daniel Regalado Full ChapterDocument51 pagesGray Hat Hacking The Ethical Hackers Handbook Sixth Edition Daniel Regalado Full Chaptereugene.poremski145100% (5)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- UntitledDocument37 pagesUntitledDevanathan ChinnasamyNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Meritlist - Combined - 2015 29.08.2015 Final PDFDocument233 pagesMeritlist - Combined - 2015 29.08.2015 Final PDFAnshul AroraNo ratings yet
- The Final Research PaperDocument47 pagesThe Final Research Paperapi-402790311No ratings yet
- Agency ArchiveDocument413 pagesAgency ArchiveAZ 211100% (3)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Cojinete Teflon - GGB-HSG-High-Load-Fiber-Reinforced-Composite-PTFE-Bearing-DatasheetDocument2 pagesCojinete Teflon - GGB-HSG-High-Load-Fiber-Reinforced-Composite-PTFE-Bearing-DatasheetneodymioNo ratings yet
- Marc A. Levitt: AuthorDocument16 pagesMarc A. Levitt: AuthorAlonso Rodriguez EscobedoNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Input Data Sheet For E-Class Record: Region Division School Name School Id School YearDocument18 pagesInput Data Sheet For E-Class Record: Region Division School Name School Id School YearRonie DacubaNo ratings yet
- Stress Diary - Identifying Causes of Short-Term Stress PDFDocument6 pagesStress Diary - Identifying Causes of Short-Term Stress PDFgggNo ratings yet
- Activity Sheet For Physical Education 3Document16 pagesActivity Sheet For Physical Education 3Elmer GornezNo ratings yet
- Pengaruh Penerapan Strategi Pelaksanaan Keluarga Terhadap Kemampuan Keluarga Merawat Pasien Halusinasi Di Kota Jambi Tahun 2017Document8 pagesPengaruh Penerapan Strategi Pelaksanaan Keluarga Terhadap Kemampuan Keluarga Merawat Pasien Halusinasi Di Kota Jambi Tahun 2017novanNo ratings yet
- Part3 Icho 11 15 PDFDocument124 pagesPart3 Icho 11 15 PDFManuel GuilhermeNo ratings yet
- SA Steam GenerationDocument6 pagesSA Steam GenerationRajagopalNo ratings yet
- Aids Introduction Related To ObstetricsDocument28 pagesAids Introduction Related To ObstetricsRoselineTigga100% (1)
- Botium Toys - Audit Scope and GoalsDocument2 pagesBotium Toys - Audit Scope and GoalsBMU WARRINo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
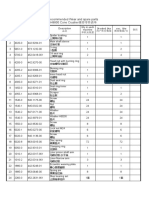
- Recommended Wear and spare parts H8800 Cone Crusher推荐零件清单Document3 pagesRecommended Wear and spare parts H8800 Cone Crusher推荐零件清单Lmf DanielNo ratings yet
- Hydro Electric Power Plant 28012019Document85 pagesHydro Electric Power Plant 28012019Rahul YadavNo ratings yet
- Miguel v. Montanez Case DigestDocument1 pageMiguel v. Montanez Case DigestMykee NavalNo ratings yet
- Fire Safety & Emergency Evacuation Plan Nicollet Public School Required by Minnesota State Fire CodeDocument5 pagesFire Safety & Emergency Evacuation Plan Nicollet Public School Required by Minnesota State Fire CodeidahssNo ratings yet
- Home Page Principles Practitioners Help Yourself Contact: Main NavigationDocument2 pagesHome Page Principles Practitioners Help Yourself Contact: Main NavigationAbdurrahmanUsmanNo ratings yet
- Substance Abuse and Psychiatric: Disordersin Prison InmatesDocument3 pagesSubstance Abuse and Psychiatric: Disordersin Prison InmatesNorberth Ioan OkrosNo ratings yet
- English - JapanDocument2 pagesEnglish - JapanJoseNo ratings yet
- Niral Network ProductsDocument7 pagesNiral Network ProductsNiral NetworksNo ratings yet
- Msds of Spray Dried LactoseDocument8 pagesMsds of Spray Dried LactoseAnandaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Wire DrawingDocument47 pagesWire DrawingKamlesh Kumar100% (3)
- Chapter 1: The Principle of NMR: Some RemindersDocument51 pagesChapter 1: The Principle of NMR: Some RemindersAkino AskNo ratings yet
- Germ LayerDocument9 pagesGerm LayerJcee EsurenaNo ratings yet
- Molecular Basis of InheritanceDocument37 pagesMolecular Basis of Inheritancechristopher lopezNo ratings yet
- Example 14refrigerationDocument2 pagesExample 14refrigerationryan williamNo ratings yet
- Chlamydia InfectionsDocument4 pagesChlamydia InfectionsPearl CalisNo ratings yet