You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Respiratory Care ModalitiesDocument5 pagesRespiratory Care ModalitiesWendy EscalanteNo ratings yet
- Concept Map Finished 2Document6 pagesConcept Map Finished 2api-352785497100% (1)
- 1 Five Year PlanDocument5 pages1 Five Year PlanPratiksha AmbedkarNo ratings yet
- Post Basic BSC Nursing: RUHS Entrance Examination 2019 Question PaperDocument29 pagesPost Basic BSC Nursing: RUHS Entrance Examination 2019 Question PaperPratiksha AmbedkarNo ratings yet
- 5 6145255034071286284Document5 pages5 6145255034071286284Pratiksha Ambedkar100% (1)
- The Individual With Functional Psychiatric Disorder: Skhizo PhrenDocument14 pagesThe Individual With Functional Psychiatric Disorder: Skhizo PhrenPratiksha AmbedkarNo ratings yet
- Tuberculosis Nursing Care Plan Ineffective Airway Clearance PDFDocument2 pagesTuberculosis Nursing Care Plan Ineffective Airway Clearance PDFPratiksha AmbedkarNo ratings yet
- Lung AbscessDocument28 pagesLung AbscessBobet ReñaNo ratings yet
- Drager Pp10 User ManualDocument2 pagesDrager Pp10 User Manualromedic36No ratings yet
- Cetak Stop Opname - AlkesDocument22 pagesCetak Stop Opname - AlkesOkto YutubNo ratings yet
- Decreasing Hospital Length of StayDocument7 pagesDecreasing Hospital Length of Staydaniel cepeda bareñoNo ratings yet
- CSE376 - Lec7 Confined SpaceDocument38 pagesCSE376 - Lec7 Confined SpaceKeith FUNo ratings yet
- Assignment 2 On Respiratory PPEDocument11 pagesAssignment 2 On Respiratory PPEAngelo SaysonNo ratings yet
- MSDS - Hella DD 2019Document10 pagesMSDS - Hella DD 2019agus cahyadiNo ratings yet
- Athletes Medical Form 1Document2 pagesAthletes Medical Form 1JEZREEL HAVANANo ratings yet
- Cameleon en PDFDocument9 pagesCameleon en PDFTurtoi AlexandruNo ratings yet
- (Advances in Delivery Science and Technology) Kevin P. O'Donnell, Hugh D. C. Smyth (Auth.), Hugh D.C. Smyth, Anthony J. Hickey (Eds.) - Controlled Pulmonary Drug Delivery - Springer-Verlag NeDocument572 pages(Advances in Delivery Science and Technology) Kevin P. O'Donnell, Hugh D. C. Smyth (Auth.), Hugh D.C. Smyth, Anthony J. Hickey (Eds.) - Controlled Pulmonary Drug Delivery - Springer-Verlag NeEnrique Dirzo MartinezNo ratings yet
- English Dialogue (Intervention) - Thalia and AgnesDocument3 pagesEnglish Dialogue (Intervention) - Thalia and AgnesElisasmitha DasilvaNo ratings yet
- 3 ClaimsDocument3 pages3 ClaimsBluishsecret WPNo ratings yet
- AX800 - Specification V 1.2 2020.2.1Document6 pagesAX800 - Specification V 1.2 2020.2.1AndresNo ratings yet
- Chest Physiotherapy - Postural DrainageDocument2 pagesChest Physiotherapy - Postural DrainageMicah MagallanoNo ratings yet
- NCP - Ineffective Breathing PatternDocument3 pagesNCP - Ineffective Breathing PatternJose Marlon CandelariaNo ratings yet
- 06 Offline Module CourseDocument15 pages06 Offline Module CourseDylan Angelo AndresNo ratings yet
- Respiratory DisordersDocument6 pagesRespiratory DisordersSusan MaglaquiNo ratings yet
- Opportunities and Challenges For Public Procurement in The First Months of The COVID 19 Pandemic Results From An Experts SurveyDocument63 pagesOpportunities and Challenges For Public Procurement in The First Months of The COVID 19 Pandemic Results From An Experts SurveyCiprian SecuNo ratings yet
- Cs2 MethodDocument48 pagesCs2 MethodMadonna SamirNo ratings yet
- Vital SignsDocument2 pagesVital SignsstaciadokNo ratings yet
- Universidad Santiago de CaliDocument3 pagesUniversidad Santiago de CaliValentina MorenoNo ratings yet
- Volume Targeted VentilationDocument4 pagesVolume Targeted VentilationAli Mohamed AbdallaNo ratings yet
- DOC044Document21 pagesDOC044danniNo ratings yet
- Manila Central University College of Medicine Department of PediatricsDocument7 pagesManila Central University College of Medicine Department of PediatricsKirstie de LunaNo ratings yet
- Fabric Softener SmartClean SDSDocument4 pagesFabric Softener SmartClean SDSAlma PustaNo ratings yet
- WHO COVID-19 Report April 28, 2020Document12 pagesWHO COVID-19 Report April 28, 2020CityNewsToronto100% (1)
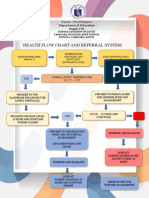
- Health Flow Chart and Referral System: Department of EducationDocument2 pagesHealth Flow Chart and Referral System: Department of EducationWendy TablaNo ratings yet
- Recommended Doses of Medications To Treat Children With An Acute Asthma ExacerbaDocument3 pagesRecommended Doses of Medications To Treat Children With An Acute Asthma Exacerbaمعاذ الشريفNo ratings yet