You might also like
- Singh2015update Incidence KDDocument6 pagesSingh2015update Incidence KDprincezettaNo ratings yet
- v07p0681 PDFDocument6 pagesv07p0681 PDFAzizaNo ratings yet
- Healthcare 10 01745Document10 pagesHealthcare 10 01745Vera El Sammah SiagianNo ratings yet
- Civ 028Document9 pagesCiv 028Deah RisbaNo ratings yet
- MainDocument15 pagesMainRobert ChristevenNo ratings yet
- Fall in AdultDocument14 pagesFall in AdultSandi IrvantaNo ratings yet
- PIIS0161642019320998Document9 pagesPIIS0161642019320998Sarah RahmawatiNo ratings yet
- International Journal of Pediatric Research Ijpr 9 111Document6 pagesInternational Journal of Pediatric Research Ijpr 9 111VsbshNo ratings yet
- Afhs2002 0860Document11 pagesAfhs2002 0860shindyNo ratings yet
- Clinical Patterns of Kawasaki Disease and Factors Associated With Echocardiography Abnormalities at Presentation Libyan ExperienceDocument7 pagesClinical Patterns of Kawasaki Disease and Factors Associated With Echocardiography Abnormalities at Presentation Libyan ExperienceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cep 2020 00955Document2 pagesCep 2020 00955AmarantoNo ratings yet
- Review Article: Kawasaki Disease: A Clinician's UpdateDocument8 pagesReview Article: Kawasaki Disease: A Clinician's UpdatePeter HoNo ratings yet
- Global Incidence and Prevalence of Autoimmune Hepatitis 1970 2023 EClinicalDocument14 pagesGlobal Incidence and Prevalence of Autoimmune Hepatitis 1970 2023 EClinicalronaldquezada038No ratings yet
- Prevalence of Vitiligo and Associated Comorbidities in KoreaDocument7 pagesPrevalence of Vitiligo and Associated Comorbidities in KoreaRatna NingsihNo ratings yet
- Pone 0269706Document13 pagesPone 0269706Meidita Annisa PurmanNo ratings yet
- American J Hematol - 2022 - Osunkwo - Burden of Disease Treatment Utilization and The Impact On Education and EmploymentDocument10 pagesAmerican J Hematol - 2022 - Osunkwo - Burden of Disease Treatment Utilization and The Impact On Education and EmploymentHijaz HijaNo ratings yet
- An Investigation Into Factors Hindering Effective Uptake of Vaccine Among Children Who Are Below Five (5) in Akinyele Local Government Area Ibadan Oyo State, NigeriaDocument14 pagesAn Investigation Into Factors Hindering Effective Uptake of Vaccine Among Children Who Are Below Five (5) in Akinyele Local Government Area Ibadan Oyo State, NigeriaCentral Asian StudiesNo ratings yet
- Kawasakidisease: Rosie ScuccimarriDocument21 pagesKawasakidisease: Rosie Scuccimarrireza ahda kadirNo ratings yet
- The Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionFrom EverandThe Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Fped 10 890767Document18 pagesFped 10 890767Feby JuwitaNo ratings yet
- Adhrence Article 1Document6 pagesAdhrence Article 1OBIOMA LILIAN OKWUONUNo ratings yet
- Evolving Trends in Infective Endocarditis in A Developing Country: A Consequence of Medical Progress?Document9 pagesEvolving Trends in Infective Endocarditis in A Developing Country: A Consequence of Medical Progress?Hassan Abdi JamaNo ratings yet
- The Current Status of KidneyTransplantationDocument7 pagesThe Current Status of KidneyTransplantationTaiwo LadapoNo ratings yet
- 1 s2.0 S2352304219300698 Main PDFDocument9 pages1 s2.0 S2352304219300698 Main PDFdioNo ratings yet
- Burden of Depression and Associated Factors Among Patients With Sickle Cell Disease in Fako Division CameroonDocument11 pagesBurden of Depression and Associated Factors Among Patients With Sickle Cell Disease in Fako Division CameroonAthenaeum Scientific PublishersNo ratings yet
- Cancers 14 02230 v2Document12 pagesCancers 14 02230 v2bisak.j.adelaNo ratings yet
- 01-Facilitators and Barriers For The Delivery and Uptake of Cervical Cancer Screening in IndonesiDocument16 pages01-Facilitators and Barriers For The Delivery and Uptake of Cervical Cancer Screening in IndonesiInggita Adinda PutriNo ratings yet
- 4Document20 pages4RobertVellaZammitNo ratings yet
- 논문원문Document7 pages논문원문Donghee LeeNo ratings yet
- BacterialmeningitisDocument9 pagesBacterialmeningitisTofik HusseinNo ratings yet
- Increasing Trends in The Incidence and PrevalenceDocument11 pagesIncreasing Trends in The Incidence and PrevalencemithapratamaaNo ratings yet
- Risk of Atrial Fibrillation According To Cancer Type: A Nationwide Population-Based StudyDocument12 pagesRisk of Atrial Fibrillation According To Cancer Type: A Nationwide Population-Based StudyBryan NguyenNo ratings yet
- Emergency Department Utilization by Californians With Sickle Cell Disease, 2005-2014Document6 pagesEmergency Department Utilization by Californians With Sickle Cell Disease, 2005-2014MateoZuluagaGomezNo ratings yet
- Severe Sepsis-Associated Morbidity and Mortality Among Critically Ill Children With CancerDocument8 pagesSevere Sepsis-Associated Morbidity and Mortality Among Critically Ill Children With CancerFaki D'pasnizerNo ratings yet
- 2021 Article 2564Document10 pages2021 Article 2564Cinthya Añazco RomeroNo ratings yet
- JIAS 2020 23 2 E25446 7pDocument7 pagesJIAS 2020 23 2 E25446 7pPeriasamy RathinasamyNo ratings yet
- Short and Long Term Outcome BBLRDocument7 pagesShort and Long Term Outcome BBLRLissaberti AmaliahNo ratings yet
- Pregnancy Outcomes in Korean Women With Ankylosing SpondylitisDocument16 pagesPregnancy Outcomes in Korean Women With Ankylosing SpondylitisDipyanalarNo ratings yet
- Prevalence and Risk Factors For ChronicDocument10 pagesPrevalence and Risk Factors For ChronicKhoirul AnamNo ratings yet
- Social Determinants of Health and Emergency Department Use Among Children With Sickle Cell DiseaseDocument4 pagesSocial Determinants of Health and Emergency Department Use Among Children With Sickle Cell DiseaseLindsay CortrightNo ratings yet
- Prevalence of Knee Osteoarthritis, Risk Factors, and Quality of Life: The Fifth Korean National Health and Nutrition Examination SurveyDocument9 pagesPrevalence of Knee Osteoarthritis, Risk Factors, and Quality of Life: The Fifth Korean National Health and Nutrition Examination SurveyTanvirNo ratings yet
- Jiaa 220Document3 pagesJiaa 220Stephanie HellenNo ratings yet
- Assessing Knowledge, Attitudes, and Practices Regarding Sickle Cell Disease Among Outpatients at Jinja Referral HospitalDocument7 pagesAssessing Knowledge, Attitudes, and Practices Regarding Sickle Cell Disease Among Outpatients at Jinja Referral HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- DamianiDocument12 pagesDamianiluis moralesNo ratings yet
- Seroprevalence of COVID-19 Infection in A Rural District of South India: A Population-Based Seroepidemiological StudyDocument11 pagesSeroprevalence of COVID-19 Infection in A Rural District of South India: A Population-Based Seroepidemiological StudySANAULLAH SULTANPURNo ratings yet
- SaudiJKidneyDisTranspl304812-2026889 053748Document7 pagesSaudiJKidneyDisTranspl304812-2026889 053748yenny handayani sihiteNo ratings yet
- SCDAC Sickle Cell Release 092015Document3 pagesSCDAC Sickle Cell Release 092015asafoabe4065No ratings yet
- Epidemi IbdDocument9 pagesEpidemi IbdShanaz NovriandinaNo ratings yet
- Assessment of Nurses' Knowledge, Attitude, Practice and Associated Factors Towards Palliative Care: in The Case of Amhara Region HospitalsDocument15 pagesAssessment of Nurses' Knowledge, Attitude, Practice and Associated Factors Towards Palliative Care: in The Case of Amhara Region HospitalsjetendraNo ratings yet
- Assessment of Knowledge of Chronic Kidney Disease PDFDocument7 pagesAssessment of Knowledge of Chronic Kidney Disease PDFمالك مناصرةNo ratings yet
- Kead 348Document9 pagesKead 348Alberto Sifuentes GiraldoNo ratings yet
- 77d8 PDFDocument7 pages77d8 PDFRosyid PrasetyoNo ratings yet
- s41598 021 88207 6 PDFDocument8 pagess41598 021 88207 6 PDFManuel ArenasNo ratings yet
- Journal Pone 0244265Document15 pagesJournal Pone 0244265Faisal YousafNo ratings yet
- Prevalence and Risk Factors of Upper Gastrointestinal Cancers Missed During Endoscopy: A Nationwide Registry-Based StudyDocument8 pagesPrevalence and Risk Factors of Upper Gastrointestinal Cancers Missed During Endoscopy: A Nationwide Registry-Based StudyDoggoboy WolfmannNo ratings yet
- Coronavirus Disease 2019 and Vaccination of Children and Adolescents - Prospects and Challenges - (ENG)Document6 pagesCoronavirus Disease 2019 and Vaccination of Children and Adolescents - Prospects and Challenges - (ENG)Handoko MuhammadNo ratings yet
- Journal Health CareDocument10 pagesJournal Health CareMeidita Annisa PurmanNo ratings yet
- Sickle Cell ServicesDocument3 pagesSickle Cell Servicesstephen X-SILVERNo ratings yet
- The Republic of Korea’s Coronavirus Disease Pandemic Response and Health System PreparednessFrom EverandThe Republic of Korea’s Coronavirus Disease Pandemic Response and Health System PreparednessNo ratings yet
- Bagian Ilmu Kesehatan Anak FK UNSRAT/ RSU. Prof. Dr. R.D. Kandou-ManadoDocument29 pagesBagian Ilmu Kesehatan Anak FK UNSRAT/ RSU. Prof. Dr. R.D. Kandou-ManadoAmarantoNo ratings yet
- ISK - Manado April 09Document83 pagesISK - Manado April 09AmarantoNo ratings yet
- Reliability and Validity of Pedsql For Portuguese Children Aged 5-7 and 8-12 YearsDocument9 pagesReliability and Validity of Pedsql For Portuguese Children Aged 5-7 and 8-12 YearsAmarantoNo ratings yet
- During The Past Week : 7. Now We Would Like To Know A Bit More About Your Epilepsy!Document3 pagesDuring The Past Week : 7. Now We Would Like To Know A Bit More About Your Epilepsy!AmarantoNo ratings yet
- Kid - KiddoKINDL - Parents - 7-17y - Additional Sub-Scale Disease - EnglishDocument2 pagesKid - KiddoKINDL - Parents - 7-17y - Additional Sub-Scale Disease - EnglishAmarantoNo ratings yet
- Kiddo - KINDL - Adolescents - 14-17y - Additional Sub-Scale Disease - EnglishDocument2 pagesKiddo - KINDL - Adolescents - 14-17y - Additional Sub-Scale Disease - EnglishAmarantoNo ratings yet
- Kid - KINDL - Children - 7-13y - Additional Sub-Scale Disease - EnglishDocument2 pagesKid - KINDL - Children - 7-13y - Additional Sub-Scale Disease - EnglishAmarantoNo ratings yet
- PEDSQLDocument4 pagesPEDSQLAmaranto100% (1)
- JP Pakai LW ScreentimeeDocument7 pagesJP Pakai LW ScreentimeeAmarantoNo ratings yet
- Questionnaire For Adolescents: There Are No Right or Wrong Answers. It's What You Think That MattersDocument3 pagesQuestionnaire For Adolescents: There Are No Right or Wrong Answers. It's What You Think That MattersAmarantoNo ratings yet
- JP 8 School ReadinessDocument8 pagesJP 8 School ReadinessAmarantoNo ratings yet
- JP 6 QuarantineDocument5 pagesJP 6 QuarantineAmarantoNo ratings yet
- JP 7 Physical Activity Parent Low High EducatedDocument11 pagesJP 7 Physical Activity Parent Low High EducatedAmarantoNo ratings yet
- Comparison of Second-Line Therapy in Ivig-Refractory Kawasaki Disease: A Systematic ReviewDocument8 pagesComparison of Second-Line Therapy in Ivig-Refractory Kawasaki Disease: A Systematic ReviewAmarantoNo ratings yet
- Kawasaki Disease: A Comprehensive Review: Kamleshun Ramphul, Stephanie Gonzalez MejiasDocument5 pagesKawasaki Disease: A Comprehensive Review: Kamleshun Ramphul, Stephanie Gonzalez MejiasAmarantoNo ratings yet
- Refractory Kawasaki Disease: C R P I DDocument2 pagesRefractory Kawasaki Disease: C R P I DAmarantoNo ratings yet
- Daftar PustakaDocument2 pagesDaftar Pustakawildantaufiq29No ratings yet
- Gastrointestinal and Liver Disease Desk ReferenceDocument16 pagesGastrointestinal and Liver Disease Desk ReferenceWahyu Ika Wardhani100% (1)
- Sri Devraj Urs Medical CollegeDocument11 pagesSri Devraj Urs Medical CollegepentagoneducationNo ratings yet
- Leaflet Sched of Doctors As of May 31, 2Document3 pagesLeaflet Sched of Doctors As of May 31, 2Philip Jay-ar DimailigNo ratings yet
- Continuous Quality Improvement ProjectDocument14 pagesContinuous Quality Improvement Projectapi-488538030No ratings yet
- NeuroDocument35 pagesNeuroFlor OMNo ratings yet
- Star Provider Directory TXDocument506 pagesStar Provider Directory TXArturo esparsaNo ratings yet
- Manual de Entrenamiento Ventilador de Anestesia Blease 8500Document69 pagesManual de Entrenamiento Ventilador de Anestesia Blease 8500Roberto Ramírez80% (5)
- Pauline Filipek - A Comparison of Live Versus Video Conditions For Measurement of Eye Contact in Infants at Age 6 Months As Red Flags' For ASDDocument1 pagePauline Filipek - A Comparison of Live Versus Video Conditions For Measurement of Eye Contact in Infants at Age 6 Months As Red Flags' For ASDAUCDNo ratings yet
- USMLE Step 2 CK Exam - Overview - Examination Content - Test Format - EligibilityDocument7 pagesUSMLE Step 2 CK Exam - Overview - Examination Content - Test Format - EligibilityJamesHowsonNo ratings yet
- Acrylic Partial DenturesDocument6 pagesAcrylic Partial DenturesCloudcynaraaNo ratings yet
- 03mb5 17 PDFDocument3 pages03mb5 17 PDFKhusnah KhauliyaNo ratings yet
- Cardiology ConsultsDocument2 pagesCardiology ConsultsjuweriyNo ratings yet
- Chu Dai Bi TagsDocument5 pagesChu Dai Bi TagsTrung Kien NguyenNo ratings yet
- E CalyptusDocument1 pageE CalyptusArdito GollerNo ratings yet
- مشروع Edited E. ColiDocument2 pagesمشروع Edited E. ColiYousef A. ZounehNo ratings yet
- Cleft Lip and Palate (Berkowitz) 3rd Ed PDFDocument966 pagesCleft Lip and Palate (Berkowitz) 3rd Ed PDFAditya SeptianNo ratings yet
- Restorations in Pediatric DentistryDocument250 pagesRestorations in Pediatric DentistrySivam Nirosan100% (2)
- ACCREDITATIONDocument62 pagesACCREDITATIONMargeYagoJulianoNo ratings yet
- Fortis Escorts HospitalDocument5 pagesFortis Escorts HospitalMike TetronNo ratings yet
- Singapore Course ProgrammeDocument3 pagesSingapore Course ProgrammeAndhika Ilmu Tak TerhinggaNo ratings yet
- DR Afshan Rehan CVDocument7 pagesDR Afshan Rehan CVArsalan AqeeqNo ratings yet
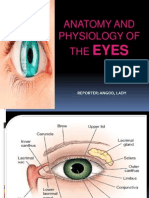
- Anatomy and Physiology of The EyesDocument20 pagesAnatomy and Physiology of The EyesLaidy Aizahlyn Indoc Angod100% (2)
- 37 - The Five Elements of HomotoxicologyDocument1 page37 - The Five Elements of HomotoxicologyRui PiresNo ratings yet
- Electobistury DT-S400Document4 pagesElectobistury DT-S400Soporte VitalNo ratings yet
- Sarvendriyanam Nayanam Pradhanam.Document25 pagesSarvendriyanam Nayanam Pradhanam.Panchajanya Kumar deeviNo ratings yet
- Baseline Vital Signs, Monitoring Devices, and History TakingDocument100 pagesBaseline Vital Signs, Monitoring Devices, and History TakingLim Jun Bin100% (1)
- PresentasiDocument30 pagesPresentasiagusNo ratings yet
- Pediatric Forensic Pathology: Limits and ControversiesDocument191 pagesPediatric Forensic Pathology: Limits and Controversieschrisr310No ratings yet
- HERNIAS in PaediatricsDocument27 pagesHERNIAS in PaediatricsHugh JacobsNo ratings yet