You might also like
- Facet Joint CapsuleDocument3 pagesFacet Joint CapsuleTrung Hiệp ĐàoNo ratings yet
- Assembling Acupuncture Points To Impart A Meaningful Neuromodulatory InputDocument2 pagesAssembling Acupuncture Points To Impart A Meaningful Neuromodulatory InputTrung Hiệp ĐàoNo ratings yet
- Extrasegmental Acupuncture Points and Autonomic FunctionDocument2 pagesExtrasegmental Acupuncture Points and Autonomic FunctionTrung Hiệp ĐàoNo ratings yet
- The Rostral Ventral Lateral Medulla: Somato-Somatic ReflexesDocument2 pagesThe Rostral Ventral Lateral Medulla: Somato-Somatic ReflexesTrung Hiệp ĐàoNo ratings yet
- Chapter 2:: Function Follows Form 29Document3 pagesChapter 2:: Function Follows Form 29Trung Hiệp ĐàoNo ratings yet
- ND NeckDocument2 pagesND NeckTrung Hiệp ĐàoNo ratings yet
- Middle Cervical GanglionDocument2 pagesMiddle Cervical GanglionTrung Hiệp ĐàoNo ratings yet
- Yin and Yang in The Modern EraDocument1 pageYin and Yang in The Modern EraTrung Hiệp ĐàoNo ratings yet
- How Acupuncture Points Affect Internal OrgansDocument2 pagesHow Acupuncture Points Affect Internal OrgansTrung Hiệp ĐàoNo ratings yet
- Sympathetic Preganglionic Levels Site of Synapse of Pre-And Post-Gan Glionic Sympathetic Neurons Course of Nociceptive Afferent Pathways Into The Central Nervous System Lungs (Including TheDocument2 pagesSympathetic Preganglionic Levels Site of Synapse of Pre-And Post-Gan Glionic Sympathetic Neurons Course of Nociceptive Afferent Pathways Into The Central Nervous System Lungs (Including TheTrung Hiệp ĐàoNo ratings yet
- The Needle-Tissue InterfaceDocument1 pageThe Needle-Tissue InterfaceTrung Hiệp ĐàoNo ratings yet
- Yin and Yang in The Modern EraDocument2 pagesYin and Yang in The Modern EraTrung Hiệp ĐàoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pump Start Up ChecklistDocument14 pagesPump Start Up ChecklistSharif Mohammad AdwanNo ratings yet
- Diagnostic Value of Non Invasive Liver Function Tests in Liver Fibrosis and Changes in These Parameters Post Metabolic SurgeryDocument7 pagesDiagnostic Value of Non Invasive Liver Function Tests in Liver Fibrosis and Changes in These Parameters Post Metabolic SurgeryTan BulNo ratings yet
- Case Presentation PBL 12 Bipolar DisorderDocument65 pagesCase Presentation PBL 12 Bipolar DisorderKim S GutierrezNo ratings yet
- UEFA Elite Club Injury StudyDocument47 pagesUEFA Elite Club Injury StudyaldoNo ratings yet
- Zinc in Human HealthDocument13 pagesZinc in Human HealthHmed Ben MohamedNo ratings yet
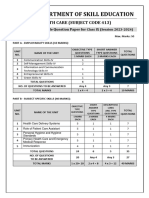
- 413 Health Care SQPDocument7 pages413 Health Care SQPAnil SarohaNo ratings yet
- Performance Checklist - Assessing The Head & Neck-1-1Document2 pagesPerformance Checklist - Assessing The Head & Neck-1-1Berlon LacsonNo ratings yet
- Jurikkes Vol 3 No 1 April 2024 Hal 70-77Document8 pagesJurikkes Vol 3 No 1 April 2024 Hal 70-77Bagus TriagungNo ratings yet
- Research Paper Chapter 1-5Document29 pagesResearch Paper Chapter 1-5SergioNo ratings yet
- Critical Care Nursing AssignmentDocument13 pagesCritical Care Nursing Assignmentiqmal irfamimi50% (2)
- Star Group Health InsuranceDocument22 pagesStar Group Health InsurancePREM NATHNo ratings yet
- Assessment Knowledge of Diabetic Foot Care Among Nursing Student at Umm Alqura University) FinalDocument13 pagesAssessment Knowledge of Diabetic Foot Care Among Nursing Student at Umm Alqura University) Finalhala yehiaNo ratings yet
- MMSU Psychosocial Assessment GuideDocument8 pagesMMSU Psychosocial Assessment GuideJohn Michael TaylanNo ratings yet
- PATHOLOGYDocument22 pagesPATHOLOGYMwanja MosesNo ratings yet
- Review of LiteratureDocument7 pagesReview of Literaturearjun singhaNo ratings yet
- Physiologic Obstetrics by APMCDocument1,091 pagesPhysiologic Obstetrics by APMCKatrina Cajigal100% (8)
- Mindfulness and Schema TherapyDocument1 pageMindfulness and Schema Therapydaitkensmith4330100% (1)
- Psychiatry Research: Brittany M Gouse, Elijah E. Boliver, Rachel Oblath, Luisa Camacho, Hannah E BrownDocument7 pagesPsychiatry Research: Brittany M Gouse, Elijah E. Boliver, Rachel Oblath, Luisa Camacho, Hannah E BrownNers EducationNo ratings yet
- Prenatal Substance Dependence AbuseDocument13 pagesPrenatal Substance Dependence Abusenursereview100% (2)
- Cardiac Cycle: BY: Makkawi .A.A. Osman B.SC, M.SC Department of Physiology Session NoDocument27 pagesCardiac Cycle: BY: Makkawi .A.A. Osman B.SC, M.SC Department of Physiology Session NoHomed OpriNo ratings yet
- Patient Satisfaction: Presented by Amaal MersalDocument48 pagesPatient Satisfaction: Presented by Amaal MersalEhab Ahmed Hussein ReyadNo ratings yet
- Guillain-Barré Syndrome: I. Anatomical and Physiological BackgroundDocument8 pagesGuillain-Barré Syndrome: I. Anatomical and Physiological BackgroundSteve ColbertNo ratings yet
- B.SC Nursing-2018-Question Papers-First Year-Microbiology FR PDFDocument1 pageB.SC Nursing-2018-Question Papers-First Year-Microbiology FR PDFSwapnil satputeNo ratings yet
- Quick Reference Guide April 2019 PDFDocument2 pagesQuick Reference Guide April 2019 PDFAaron ShokarNo ratings yet
- PPK DOKTER GIGI EDIT Bareng (23102014) .2 PDFDocument10 pagesPPK DOKTER GIGI EDIT Bareng (23102014) .2 PDFeatmyfleasNo ratings yet
- Sphygmomanometer Calibration Why, How and How Often?: Australian Family Physician November 2007Document5 pagesSphygmomanometer Calibration Why, How and How Often?: Australian Family Physician November 2007jlgallardoNo ratings yet
- Final Research GumamleaDocument29 pagesFinal Research GumamleaShiela Mae LiwanagNo ratings yet
- Standard Methods For Apis Mellifera Pest and Pathogen Research IntroductionDocument4 pagesStandard Methods For Apis Mellifera Pest and Pathogen Research IntroductionKátia Peres GramachoNo ratings yet
- 7297 19768 4 PBDocument5 pages7297 19768 4 PBpujiindah lestariNo ratings yet
- Introduction To Tungs Acupuncture PDFDocument323 pagesIntroduction To Tungs Acupuncture PDFBala Kiran Gaddam98% (48)