You might also like
- Knots in Orthopedic Surgery: Open and Arthroscopic TechniquesFrom EverandKnots in Orthopedic Surgery: Open and Arthroscopic TechniquesUmut AkgunNo ratings yet
- Removal of Ear, Nose andDocument4 pagesRemoval of Ear, Nose andandinNo ratings yet
- Umbilicalherniarepair: Overview of Approaches and Review of LiteratureDocument16 pagesUmbilicalherniarepair: Overview of Approaches and Review of LiteratureVictor Matias BarriosNo ratings yet
- Cleft Palate Repair, Gingivoperiosteoplasty and Alveolar Bone GraftingDocument10 pagesCleft Palate Repair, Gingivoperiosteoplasty and Alveolar Bone GraftingAndrés Faúndez TeránNo ratings yet
- 11 2 34 PDFDocument3 pages11 2 34 PDFAgusNo ratings yet
- International Journal of Surgery: Sri Vengadesh Gopal, Achuthan WarrierDocument4 pagesInternational Journal of Surgery: Sri Vengadesh Gopal, Achuthan WarrierRon Java FantillanNo ratings yet
- Indications Plexus Reconstr OBPPDocument8 pagesIndications Plexus Reconstr OBPP2w8qg5qwhdNo ratings yet
- 27720150561679Document7 pages27720150561679apryanadarNo ratings yet
- Intimate Examinations and The Use of Chaperones: WWW - Rcr.ac - UkDocument14 pagesIntimate Examinations and The Use of Chaperones: WWW - Rcr.ac - UkMirza BaigNo ratings yet
- Midterm Ngt InsertionDocument5 pagesMidterm Ngt InsertionMaria Kyla VicenteNo ratings yet
- The Digital Rectal ExaminationDocument2 pagesThe Digital Rectal ExaminationGabriela GalvezNo ratings yet
- 0 OP Techniques General Surgery Superficial Parotidectomy OLSEN EXCELLENTDocument13 pages0 OP Techniques General Surgery Superficial Parotidectomy OLSEN EXCELLENTmuhammad ishaqueNo ratings yet
- The Use of Paraglossal Straight Blade Laryngoscopy in Difficult Tracheal IntubationDocument9 pagesThe Use of Paraglossal Straight Blade Laryngoscopy in Difficult Tracheal IntubationJset SixthousandNo ratings yet
- Pediatric Protrusion Mentioned,: Robert M.D. CityDocument2 pagesPediatric Protrusion Mentioned,: Robert M.D. Citybouchra8blsNo ratings yet
- Abdominal Incisions and Sutures in Obstetrics and GynaecologyDocument6 pagesAbdominal Incisions and Sutures in Obstetrics and GynaecologyFebyan AbotNo ratings yet
- Teknik Frenectomy Miller 2020Document4 pagesTeknik Frenectomy Miller 2020yufita fitrianiNo ratings yet
- Clinical Orthopaedic Examination-1 PDFDocument334 pagesClinical Orthopaedic Examination-1 PDFEmil Cotenescu100% (9)
- Arnold L. Freedman, Marc D. Stein, Daniel B. Schneider.Document5 pagesArnold L. Freedman, Marc D. Stein, Daniel B. Schneider.Gloria SequeiraNo ratings yet
- Warthins Tumorof Parotid GlandDocument5 pagesWarthins Tumorof Parotid GlandWahyuni NaharuddinNo ratings yet
- Raoul Tubiana - Jean-Michel Thomine - Evelyn Mackin - F Brunelli - Examination of The Hand and Wrist-CRC PressDocument406 pagesRaoul Tubiana - Jean-Michel Thomine - Evelyn Mackin - F Brunelli - Examination of The Hand and Wrist-CRC PressMaricruzhdezaNo ratings yet
- Journal Plastic - Thenar FlapDocument4 pagesJournal Plastic - Thenar FlapMuhammad WartonoNo ratings yet
- CORMACK, LEHANE - 1984 - Difficult Tracheal Intubation in ObstetricsDocument7 pagesCORMACK, LEHANE - 1984 - Difficult Tracheal Intubation in ObstetricsMubeenRahmanNo ratings yet
- Surgical Techniques in Primary Inguinal Hernia RepairDocument7 pagesSurgical Techniques in Primary Inguinal Hernia RepairNuno AzenhaNo ratings yet
- Urinary Catheterization Procedures With RationaleDocument10 pagesUrinary Catheterization Procedures With RationaleKaye NaigNo ratings yet
- Laparoscopic Hernia Repair in Neonates, Infants and ChildrenDocument9 pagesLaparoscopic Hernia Repair in Neonates, Infants and ChildrenErick OematanNo ratings yet
- Indications and The Diagnosis For Fixed Partial Denture ProsthesisDocument7 pagesIndications and The Diagnosis For Fixed Partial Denture ProsthesisDaniel Espinoza EspinozaNo ratings yet
- Eyelid DisordersDocument6 pagesEyelid DisordersCamilo PerezNo ratings yet
- 295 QsDocument3 pages295 Qsujangketul62No ratings yet
- 3dmax Light Mesh: Technique GuideDocument12 pages3dmax Light Mesh: Technique GuidenautilixxNo ratings yet
- Morphological Study On Torus Palatinus in Adult Human SkullsDocument4 pagesMorphological Study On Torus Palatinus in Adult Human SkullsOttofianus Alvedo Hewick KalangiNo ratings yet
- SteinerDocument23 pagesSteinerAlejandra Zambrano ValeroNo ratings yet
- Rle 107 MTDocument15 pagesRle 107 MTKrizia Claire Marie RedondoNo ratings yet
- Rapid Palatal Expansion in The Young Adult A Case Report: January 2015Document7 pagesRapid Palatal Expansion in The Young Adult A Case Report: January 2015AomChanumpornNo ratings yet
- Clin Experimental Optometry - 2008 - Clinical Medicine in Optometric Practice 2nd EditionDocument2 pagesClin Experimental Optometry - 2008 - Clinical Medicine in Optometric Practice 2nd EditionnicolamihaiuNo ratings yet
- Closed Rhinoplasty The Next Generation - Paul J OKeeffe (2019)Document107 pagesClosed Rhinoplasty The Next Generation - Paul J OKeeffe (2019)poly_paparas100% (1)
- Endodontic SurgeryDocument16 pagesEndodontic SurgeryauntymayaNo ratings yet
- 2014-08-13 Suture Presentation FINAL - SlidesDocument13 pages2014-08-13 Suture Presentation FINAL - SlidesMariana HernandezNo ratings yet
- 2s2022 Ncm109 Rle Learn Mat 1Document18 pages2s2022 Ncm109 Rle Learn Mat 1Guia SalandananNo ratings yet
- Williamson 2014Document7 pagesWilliamson 2014scribd mendeleyNo ratings yet
- Guideline No. 412 Laparoscopic Entry For Gynexological SurgeryDocument16 pagesGuideline No. 412 Laparoscopic Entry For Gynexological SurgeryRaúl MartínezNo ratings yet
- Foresta 2014Document14 pagesForesta 2014stoia_sebiNo ratings yet
- ASSISTING IN BONE MARROW ASPIRATION (2) .Doc Revised. ADocument9 pagesASSISTING IN BONE MARROW ASPIRATION (2) .Doc Revised. ARiza Angela BarazanNo ratings yet
- Histopathology Grossing ProceduresDocument14 pagesHistopathology Grossing ProceduresNico Loko100% (1)
- Editorial: Ó 2002 Blackwell Science LTDDocument5 pagesEditorial: Ó 2002 Blackwell Science LTDpradeep danielNo ratings yet
- Levitt 2002Document7 pagesLevitt 2002Diego ReyNo ratings yet
- Alar Lift: Sail Excision Technique For Alar Overhanging in The Middle Eastern NoseDocument5 pagesAlar Lift: Sail Excision Technique For Alar Overhanging in The Middle Eastern NosejerryimNo ratings yet
- 1 Suhasini SonavdekarDocument6 pages1 Suhasini SonavdekarArlia orohNo ratings yet
- How - To - Determine - Gestational - Age - of - An - Equine - Preg Mcdonell 2006Document7 pagesHow - To - Determine - Gestational - Age - of - An - Equine - Preg Mcdonell 2006kaathydanieelaNo ratings yet
- Diagnostic Laparoscopy: Surgical Endoscopy February 2004Document6 pagesDiagnostic Laparoscopy: Surgical Endoscopy February 2004carmenNo ratings yet
- History Taking: Practical 1 InstructionDocument12 pagesHistory Taking: Practical 1 InstructionDimsyafelNo ratings yet
- ABRAVAS 2 de 9 - Divers 1999 - Reptile EndosDocument8 pagesABRAVAS 2 de 9 - Divers 1999 - Reptile EndosCamilo SantanderNo ratings yet
- Palatally Impacted CaninesDocument5 pagesPalatally Impacted CaninesMoisés MartinsNo ratings yet
- PerforasiDocument3 pagesPerforasiEinz Nur Amalyah IdrusNo ratings yet
- Draping of Tibia: Sandwich TechniqueDocument3 pagesDraping of Tibia: Sandwich Techniquebagus lazuardiNo ratings yet
- Checklist For Vaginal ExaminationDocument7 pagesChecklist For Vaginal ExaminationjoaguilarNo ratings yet
- Invited Discussion On: Concentrated Growth Factors Extracted From Blood Plasma Used To Repair Nasal Septal Mucosal Defect After RhinoplastyDocument2 pagesInvited Discussion On: Concentrated Growth Factors Extracted From Blood Plasma Used To Repair Nasal Septal Mucosal Defect After RhinoplastyHiktor TomNo ratings yet
- Dorsal Ovariectomy in RodentsDocument5 pagesDorsal Ovariectomy in RodentsJavier OjedaNo ratings yet
- Evisceration With Autogenous Scleral Graft and Bioceramic Implantation Within The Modified Scleral Shell 133 Cases Over 17 YearsDocument6 pagesEvisceration With Autogenous Scleral Graft and Bioceramic Implantation Within The Modified Scleral Shell 133 Cases Over 17 YearsSaraelsy MonterrosoNo ratings yet
- Omphalolith Surgical ExtractionDocument2 pagesOmphalolith Surgical ExtractionWei Sheng ChongNo ratings yet
- PerikondritisDocument5 pagesPerikondritisRay RamadhanNo ratings yet
- Urolithiasis - Metabolic Considerations: Case 1Document2 pagesUrolithiasis - Metabolic Considerations: Case 1HardiTariqHammaNo ratings yet
- Urology News Jul Aug 2016 Spot TestDocument2 pagesUrology News Jul Aug 2016 Spot TestHardiTariqHammaNo ratings yet
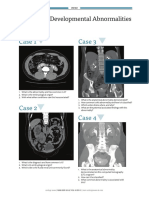
- Case 1 Case 3: Technology - Part 1Document2 pagesCase 1 Case 3: Technology - Part 1HardiTariqHammaNo ratings yet
- Uroma14 Spot Test NewDocument2 pagesUroma14 Spot Test NewHardiTariqHammaNo ratings yet
- Prostate Cancer MRI and Biopsy Spot TestDocument2 pagesProstate Cancer MRI and Biopsy Spot TestHardiTariqHammaNo ratings yet
- Urology Sample MCQ Exam eDocument2 pagesUrology Sample MCQ Exam eHardiTariqHammaNo ratings yet
- Surgical Strategies in Endourology For Stone DiseaseDocument291 pagesSurgical Strategies in Endourology For Stone DiseaseHardiTariqHammaNo ratings yet
- Registration for HoLEP Day Surgery CourseDocument2 pagesRegistration for HoLEP Day Surgery CourseHardiTariqHammaNo ratings yet
- Uroja14 Spot Test NewDocument2 pagesUroja14 Spot Test NewHardiTariqHammaNo ratings yet
- UROLOGY OSCE Skills English NT Version 2Document1 pageUROLOGY OSCE Skills English NT Version 2HardiTariqHammaNo ratings yet
- Uroma16 Spot Test 2Document2 pagesUroma16 Spot Test 2HardiTariqHammaNo ratings yet
- A. Congenital Adrenal HyperplasiaDocument5 pagesA. Congenital Adrenal HyperplasiasewmehondesalegnNo ratings yet
- Urology News Jul Aug 2016 Spot TestDocument2 pagesUrology News Jul Aug 2016 Spot TestHardiTariqHammaNo ratings yet
- Uromj14 Spot Test NewDocument2 pagesUromj14 Spot Test NewHardiTariqHammaNo ratings yet
- A. Congenital Adrenal HyperplasiaDocument5 pagesA. Congenital Adrenal HyperplasiasewmehondesalegnNo ratings yet
- EBU Summative Assessments in UrologyDocument60 pagesEBU Summative Assessments in UrologyHardiTariqHammaNo ratings yet
- Research Protocol Form, Approval Deraw DR - 1Document12 pagesResearch Protocol Form, Approval Deraw DR - 1HardiTariqHammaNo ratings yet
- Urethral Pathology: Case 1 Case 2Document2 pagesUrethral Pathology: Case 1 Case 2HardiTariqHammaNo ratings yet
- 4 5787572421108171420 PDFDocument62 pages4 5787572421108171420 PDFnanda1al1humairahNo ratings yet
- Urology OSCEDocument10 pagesUrology OSCEHardiTariqHammaNo ratings yet
- A. Congenital Adrenal HyperplasiaDocument5 pagesA. Congenital Adrenal HyperplasiasewmehondesalegnNo ratings yet
- Osces For Medical Students, Volume 2 Second EditionDocument41 pagesOsces For Medical Students, Volume 2 Second EditionNaeem Khan100% (3)
- Radiology Quiz: by Jane BelfieldDocument4 pagesRadiology Quiz: by Jane BelfieldHardiTariqHammaNo ratings yet
- LUTS Spot TestDocument2 pagesLUTS Spot TestHardiTariqHamma100% (1)
- Deadly Kidney Infection: Understanding Emphysematous Pyelonephritis (EPNDocument31 pagesDeadly Kidney Infection: Understanding Emphysematous Pyelonephritis (EPNHardiTariqHammaNo ratings yet
- Neurourology: Case 1 Case 3Document2 pagesNeurourology: Case 1 Case 3HardiTariqHammaNo ratings yet
- Uropathology: What's The Diagnosis?: Case 1 Case 2Document2 pagesUropathology: What's The Diagnosis?: Case 1 Case 2HardiTariqHammaNo ratings yet
- Paediatric Urology - Peno-Scrotal: Case 1 Case 2Document2 pagesPaediatric Urology - Peno-Scrotal: Case 1 Case 2HardiTariqHammaNo ratings yet
- Continuing Medical Education: CME Multiple Choice QuestionsDocument1 pageContinuing Medical Education: CME Multiple Choice QuestionsHardiTariqHammaNo ratings yet
- Renal Quiz (12.8.2017)Document3 pagesRenal Quiz (12.8.2017)HardiTariqHammaNo ratings yet
- Saqeeb PPT LiqueurDocument21 pagesSaqeeb PPT LiqueurSæqéëb Æl HæssåñNo ratings yet
- Assignment 6Document2 pagesAssignment 6Rishabh MelwankiNo ratings yet
- The Etherington BrothersDocument30 pagesThe Etherington Brotherstoninho_6660% (1)
- Liturgical Music For LentDocument11 pagesLiturgical Music For LentShirly Benedictos100% (1)
- New Holland E55Bx Tier 4 Compact Hydraulic Excavator Service Repair ManualDocument21 pagesNew Holland E55Bx Tier 4 Compact Hydraulic Excavator Service Repair ManualggjjjjotonesNo ratings yet
- MSC Logic Self Study 2019 CompleteDocument88 pagesMSC Logic Self Study 2019 CompleteAlyssa RenataNo ratings yet
- Negotiation Self-Assessment and Vision Report - by Umang DharDocument1 pageNegotiation Self-Assessment and Vision Report - by Umang Dharumangdhar8No ratings yet
- Well Construction Journal - May/June 2014Document28 pagesWell Construction Journal - May/June 2014Venture PublishingNo ratings yet
- Prabuddha Bharata June10Document58 pagesPrabuddha Bharata June10talk2ankitNo ratings yet
- Unimac Technical Specifications UY180 UY240 UY280Document2 pagesUnimac Technical Specifications UY180 UY240 UY280mairimsp2003No ratings yet
- Awesome Info Lock PickingDocument19 pagesAwesome Info Lock PickingApparatchiki310100% (7)
- Analysis Report Bhuwan BhaskarDocument29 pagesAnalysis Report Bhuwan BhaskarKshitiz LamichhaneNo ratings yet
- Case Study - BIG HIT ENTERTAINMENT AND BTS: K-POP REACHES FOR A GLOBAL BREAKTHROUGHDocument9 pagesCase Study - BIG HIT ENTERTAINMENT AND BTS: K-POP REACHES FOR A GLOBAL BREAKTHROUGHJENEUSE JADE TAGANASNo ratings yet
- Improving Student Vocabulary with Extensive ReadingDocument2 pagesImproving Student Vocabulary with Extensive ReadingSariayumarthatilaarNo ratings yet
- Remedial Law REVIEWER Atty. Tranquil SalvadorDocument61 pagesRemedial Law REVIEWER Atty. Tranquil SalvadorDPMPascua100% (1)
- U2000 & PRS Operation Introduce V1.0Document25 pagesU2000 & PRS Operation Introduce V1.0Nam PhamNo ratings yet
- Horno Industrial HC1 v1.1Document30 pagesHorno Industrial HC1 v1.1Cristian urielNo ratings yet
- Bioworld Naruto Classic Uzumaki Naruto Cosplay Zip-Up Hoodie, Multicolored, Medium Amazon - Ca Clothing, Shoes & AccessoriesDocument1 pageBioworld Naruto Classic Uzumaki Naruto Cosplay Zip-Up Hoodie, Multicolored, Medium Amazon - Ca Clothing, Shoes & AccessoriestonydidlyNo ratings yet
- Describing LearnersDocument29 pagesDescribing LearnersSongül Kafa67% (3)
- DLP Reading Comprehension 15th SeptemberDocument3 pagesDLP Reading Comprehension 15th SeptemberHanaa ElmostaeenNo ratings yet
- VOL. 208, MAY 7, 1992 487 Perla Compania de Seguros, Inc. vs. Court of AppealsDocument9 pagesVOL. 208, MAY 7, 1992 487 Perla Compania de Seguros, Inc. vs. Court of AppealsdanexrainierNo ratings yet
- Around The DubaiDocument11 pagesAround The DubaiGayane HovhannisyanNo ratings yet
- Wax Rolls For Your Success: Yarn Yearns For The One and OnlyDocument9 pagesWax Rolls For Your Success: Yarn Yearns For The One and Onlyangga widayantoNo ratings yet
- PSMB Certified Trainer Curriculum StructureDocument19 pagesPSMB Certified Trainer Curriculum StructureFlankerSparrowNo ratings yet
- Chapter 1:: Grammatical Description of English, Basic TermsDocument6 pagesChapter 1:: Grammatical Description of English, Basic Termsleksandra1No ratings yet
- Catalogo Tecnico Toyota BT Staxio P Series SPE120 200Document4 pagesCatalogo Tecnico Toyota BT Staxio P Series SPE120 200Asesor ComercialNo ratings yet
- Wound Healing PhasesDocument27 pagesWound Healing PhasesAnil BasnetNo ratings yet
- ARTS8 Q4 MOD2Document32 pagesARTS8 Q4 MOD2eoghannolascoNo ratings yet
- Unit 4 Reading Exercise 2Document6 pagesUnit 4 Reading Exercise 2Ivan TamaNo ratings yet