You might also like
- General Work PermitDocument1 pageGeneral Work PermitManish Chandani75% (8)
- Electrical Isolation PermitDocument2 pagesElectrical Isolation Permitsindarth raveendrakrishnan100% (9)
- General Work PermitDocument1 pageGeneral Work PermitJohn Shane100% (5)
- Ron Weasley: The Wizard Boy Crochet PatternDocument24 pagesRon Weasley: The Wizard Boy Crochet PatternElizabeth Campos93% (14)
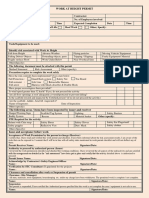
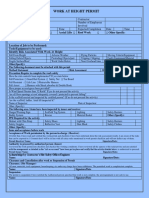
- Work at Height Permit FormDocument2 pagesWork at Height Permit FormYounis Khan76% (17)
- Confined Space Permit PDFDocument2 pagesConfined Space Permit PDFrashid zaman100% (1)
- Confined Space Entry Procedure WorksheetDocument5 pagesConfined Space Entry Procedure WorksheetToma AdrianaNo ratings yet
- Work at Height Permit FormDocument2 pagesWork at Height Permit FormYounis Khan76% (17)
- Excavation Permit FormDocument2 pagesExcavation Permit FormNash C. Usop100% (1)
- Pressure Test Work PermitDocument2 pagesPressure Test Work PermitMd Abdul Raja83% (6)
- Cold Work Permit: The Following Areas / Items Have Been Inspected by Issuer and ReceiverDocument2 pagesCold Work Permit: The Following Areas / Items Have Been Inspected by Issuer and Receiversindarth raveendrakrishnan100% (6)
- Working at HeightsDocument2 pagesWorking at HeightsDoo PLTGU100% (1)
- General Work PermitDocument2 pagesGeneral Work PermitAmol Kamble100% (1)
- Excavation Permit FormDocument2 pagesExcavation Permit FormKarim KachourNo ratings yet
- Call of Cthulhu 7e - Nakuko - The Weeping ChildDocument34 pagesCall of Cthulhu 7e - Nakuko - The Weeping ChildGema Ortega62% (13)
- Heigh Work Pemit - BlueDocument2 pagesHeigh Work Pemit - BlueAravind Babu Dasari100% (6)
- Confined Space Entry PermitDocument2 pagesConfined Space Entry Permitsindarth raveendrakrishnan100% (1)
- Cold Work Permit: The Following Areas / Items Have Been Inspected by Issuer and ReceiverDocument15 pagesCold Work Permit: The Following Areas / Items Have Been Inspected by Issuer and ReceiverSyed Amjad100% (2)
- Electrical Permit (Isolation) FormDocument2 pagesElectrical Permit (Isolation) FormNassim Akrouche100% (1)
- Permit For Working at HeightDocument1 pagePermit For Working at HeightMohit Bhadauria100% (1)
- PTW Hot Work Uoko3aDocument3 pagesPTW Hot Work Uoko3aUmair KhanNo ratings yet
- HSE Induction RecordDocument2 pagesHSE Induction RecordWinnie Eldama100% (2)
- Permit To Excavate: Section - I Contact DetailsDocument1 pagePermit To Excavate: Section - I Contact DetailsBig Zaddy0% (1)
- Excavation Work PermitDocument1 pageExcavation Work PermitKhadar BashaNo ratings yet
- Reebok AssignmentDocument6 pagesReebok Assignmentpragyanbhatt100% (1)
- Hot Work permit-REDDocument2 pagesHot Work permit-REDAravind Babu Dasari100% (1)
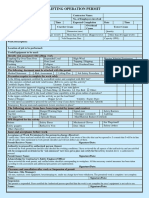
- Lifting Operation PermitDocument2 pagesLifting Operation Permitsindarth raveendrakrishnan100% (1)
- Excavation Permit: The Following Areas / Items Have Been Inspected by Issuer and ReceiverDocument2 pagesExcavation Permit: The Following Areas / Items Have Been Inspected by Issuer and Receiversindarth raveendrakrishnanNo ratings yet
- Work at Height Permit Form-2020Document2 pagesWork at Height Permit Form-2020Ebrahsm Elshenawy100% (1)
- Cold Work permit-WHITEDocument2 pagesCold Work permit-WHITEAravind Babu Dasari100% (1)
- Hot Work Permit: Welding Bracing/Cutting/Grinding/SolderingDocument2 pagesHot Work Permit: Welding Bracing/Cutting/Grinding/Solderingsindarth raveendrakrishnan100% (4)
- Excavation permit-1-GREENDocument2 pagesExcavation permit-1-GREENAravind Babu Dasari100% (1)
- Electrially Energized Area Entry PermitDocument1 pageElectrially Energized Area Entry PermitShahrukh Faizan AhmedNo ratings yet
- 05 - Work at Height PermitDocument1 page05 - Work at Height Permitwinston11100% (1)
- Electrical (Islation) Permit-YELLOWDocument2 pagesElectrical (Islation) Permit-YELLOWAravind Babu Dasari50% (2)
- 06 - Hot Work PermitDocument1 page06 - Hot Work Permitwinston11No ratings yet
- EHSWP004 - Hot Work Permit PDFDocument2 pagesEHSWP004 - Hot Work Permit PDFRand raiNo ratings yet
- General Work Permit FormatDocument1 pageGeneral Work Permit FormatprabhuNo ratings yet
- Lifting Operation PermitDocument2 pagesLifting Operation PermitFMU KSA100% (2)
- General Work Permit R1Document1 pageGeneral Work Permit R1Muthu AyyanarNo ratings yet
- Permit No:: Permit To Work-General WorkDocument3 pagesPermit No:: Permit To Work-General Workkumar kannanNo ratings yet
- Bhate & Raje Construction Co. Pvt. LTD: Electrical Work PermitDocument1 pageBhate & Raje Construction Co. Pvt. LTD: Electrical Work Permitvinayak salve100% (1)
- VR-ForM-F06.10 (Hot Work Permit Request Form)Document1 pageVR-ForM-F06.10 (Hot Work Permit Request Form)imtz2013No ratings yet
- Hot Works PermitDocument1 pageHot Works PermitOwainNo ratings yet
- Permit To Work FormsDocument8 pagesPermit To Work FormsMarc Vincent SeñorinNo ratings yet
- Hot Work Permit: This Permit Is Not Valid Unless All Appropriate Fields Are CompletedDocument2 pagesHot Work Permit: This Permit Is Not Valid Unless All Appropriate Fields Are CompletedEl Saleh newcapital100% (1)
- FORM-03-OHSE-08 General Work Permit (GWP)Document2 pagesFORM-03-OHSE-08 General Work Permit (GWP)Fadil MuhammadNo ratings yet
- Hot Work PermitDocument1 pageHot Work PermitManesh MNo ratings yet
- 06-F03 Ohs Introduction & Induction: Safety Induction Training Check-ListDocument2 pages06-F03 Ohs Introduction & Induction: Safety Induction Training Check-ListSn AhsanNo ratings yet
- Permit To Work at HeightsDocument2 pagesPermit To Work at HeightsRj Hush Esguerra100% (1)
- 088 - Work Permit FormDocument1 page088 - Work Permit FormmashanghNo ratings yet
- Health and Safety Induction ChecklistDocument2 pagesHealth and Safety Induction ChecklistYathawan Nair ThamutharamNo ratings yet
- PermitDocument8 pagesPermitSubhransu Mohapatra100% (1)
- Weekly Monthly Performance Report - Jerin Sam KurianDocument5 pagesWeekly Monthly Performance Report - Jerin Sam Kurianjerin sam kurianNo ratings yet
- HSE-P-07 Work Permit Procedure Issue 2.1Document30 pagesHSE-P-07 Work Permit Procedure Issue 2.1eng20072007100% (1)
- Permit To Work EOH-SP-FORM 531.01Document2 pagesPermit To Work EOH-SP-FORM 531.01Brad EubankNo ratings yet
- HSE Violation & PenaltiesDocument5 pagesHSE Violation & PenaltiesVladimir Radovanovic100% (1)
- Hot Work Permits: Corporate Environment Safety & HealthDocument17 pagesHot Work Permits: Corporate Environment Safety & HealthBv Rao100% (1)
- Work at HeightDocument1 pageWork at HeightVikas Yamagar100% (2)
- Form-58 Confined Space Entry LogDocument1 pageForm-58 Confined Space Entry LogRajesh Kumar SinghNo ratings yet
- Excavation Work PermitDocument2 pagesExcavation Work Permitmuhammad.younisNo ratings yet
- Excavation Permit FormDocument2 pagesExcavation Permit FormazozinlcNo ratings yet
- Cold Work Permit Form 2Document2 pagesCold Work Permit Form 2azozinlcNo ratings yet
- PTW Rev1@011122Document2 pagesPTW Rev1@011122Che ZahirNo ratings yet
- MOM Attendence 3002Document1 pageMOM Attendence 3002Younis KhanNo ratings yet
- EF-SSEMR-M-3009 - Weekly Safety Minutes of Meeting (WS-MOM)Document1 pageEF-SSEMR-M-3009 - Weekly Safety Minutes of Meeting (WS-MOM)Younis KhanNo ratings yet
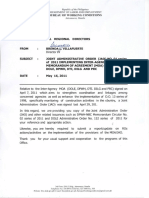
- Joint Administrative Order Construction SafetyDocument6 pagesJoint Administrative Order Construction SafetyYounis KhanNo ratings yet
- Tools and Equipment Safety PrintDocument4 pagesTools and Equipment Safety PrintYounis KhanNo ratings yet
- Ethyl Acetate MSDS: Section 1: Chemical Product and Company IdentificationDocument6 pagesEthyl Acetate MSDS: Section 1: Chemical Product and Company IdentificationYounis KhanNo ratings yet
- XD Sale June 2018Document165 pagesXD Sale June 2018Younis KhanNo ratings yet
- CM BannuDocument8 pagesCM BannuYounis KhanNo ratings yet
- Civil Shop Drawing StatusDocument46 pagesCivil Shop Drawing StatusYounis KhanNo ratings yet
- Data Sheet Gemini Tailoring AssistantDocument1 pageData Sheet Gemini Tailoring AssistantAndreea CastraseNo ratings yet
- Starters-Lesson 15 13.01.23 at The Beach and DeterminersDocument6 pagesStarters-Lesson 15 13.01.23 at The Beach and DeterminersThe English AcademyNo ratings yet
- Joining AmigurumiDocument6 pagesJoining AmigurumiBarbara Magdalena PitekNo ratings yet
- GS TG4 PrintableTest U05Document5 pagesGS TG4 PrintableTest U05Minh PhuongNo ratings yet
- 2 CHỨC NĂNG GIAO TIẾPDocument18 pages2 CHỨC NĂNG GIAO TIẾPBích Phạm Thị NgọcNo ratings yet
- Candidate A: Instructions To Candidates: Task A: Individual PresentationDocument8 pagesCandidate A: Instructions To Candidates: Task A: Individual Presentationwan333No ratings yet
- OSHA - Heat and Cold StressDocument5 pagesOSHA - Heat and Cold StressCarlos Henrique diasNo ratings yet
- Infection Control in DentistryDocument69 pagesInfection Control in DentistryShahrukh ali khanNo ratings yet
- Mapeh7 Week 1 Quarter 3Document54 pagesMapeh7 Week 1 Quarter 3joan ranchesNo ratings yet
- Top Notch 1 Unit 7-8 Test: Name: DateDocument6 pagesTop Notch 1 Unit 7-8 Test: Name: DateÁngel Alexander Zelaya López100% (1)
- Work-Based Training Plan 2.2.1Document3 pagesWork-Based Training Plan 2.2.1Roy CubilNo ratings yet
- Knit Hoodie Dog Coat - Knit: S 10" (25.5 CM) 18 22 S 1Document2 pagesKnit Hoodie Dog Coat - Knit: S 10" (25.5 CM) 18 22 S 1Keila SarayNo ratings yet
- Men S Colour Trend Concepts A W 21 22Document18 pagesMen S Colour Trend Concepts A W 21 22Raquel Mantovani0% (1)
- Customs and Traditions Uniforms Atls - : O Work in Pairs and Discuss The Following QuestionsDocument7 pagesCustoms and Traditions Uniforms Atls - : O Work in Pairs and Discuss The Following QuestionsJoaco RabinoNo ratings yet
- De Thi Khao Sat Chat Luong Dau Nam Mon Tieng Anh Lop 9 Nam 2020 2021Document11 pagesDe Thi Khao Sat Chat Luong Dau Nam Mon Tieng Anh Lop 9 Nam 2020 2021MinhNgoc HoangthiNo ratings yet
- Overgeared Vol 34Document390 pagesOvergeared Vol 34Jomari YlanaNo ratings yet
- Ae2 Itb 2ano GabaritoDocument7 pagesAe2 Itb 2ano GabaritoSandra M SilvaNo ratings yet
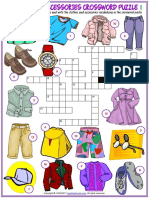
- Clothes and Accessories Vocabulary Esl Crossword Puzzle Worksheets For Kids PDFDocument6 pagesClothes and Accessories Vocabulary Esl Crossword Puzzle Worksheets For Kids PDFCarolina Cheptenari0% (1)
- Wrong NumberDocument161 pagesWrong NumberMary-Anne SueNo ratings yet
- Nike Consumer Attitude StudyDocument27 pagesNike Consumer Attitude StudyPriya dharshiniNo ratings yet
- Animal Prints - The Pattern Trend For Women's KnitwearDocument10 pagesAnimal Prints - The Pattern Trend For Women's KnitwearJoao CADILHENo ratings yet
- A Detailed Lesson Plan in English 1 DateDocument3 pagesA Detailed Lesson Plan in English 1 DateRhoma P. Tadeja100% (5)
- And Today You Anniversary Special by James WylderDocument153 pagesAnd Today You Anniversary Special by James WylderJohn SmithNo ratings yet
- Sarwat Halima Saima Habib Sadia AminDocument51 pagesSarwat Halima Saima Habib Sadia AminMikaScripnicNo ratings yet
- Morning Afternoon EveningDocument4 pagesMorning Afternoon EveningLaura BeltranNo ratings yet
- Free Adaptation From "THE TAMING OF THE SHREW" by William ShakespeareDocument29 pagesFree Adaptation From "THE TAMING OF THE SHREW" by William ShakespeareLorenzo Di DioNo ratings yet
- H.E. 6-Week 3 Sewing Tools LECTUREDocument30 pagesH.E. 6-Week 3 Sewing Tools LECTUREChezca CumilangNo ratings yet