You might also like
- The Mini-Guide To Sacred Codes and SwitchwordsDocument99 pagesThe Mini-Guide To Sacred Codes and SwitchwordsJason Alex100% (9)
- 2010 - Caliber JEEP BOITE T355Document484 pages2010 - Caliber JEEP BOITE T355thierry.fifieldoutlook.comNo ratings yet
- GC 1999 03 Minas BrethilDocument5 pagesGC 1999 03 Minas BrethilErszebethNo ratings yet
- Fast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseFrom EverandFast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseNo ratings yet
- 4-7 The Law of Sines and The Law of Cosines PDFDocument40 pages4-7 The Law of Sines and The Law of Cosines PDFApple Vidal100% (1)
- Business Continuity Generaly Accepted Practices GAP v2.1 (Disaster Recovery Journal 2015) PDFDocument140 pagesBusiness Continuity Generaly Accepted Practices GAP v2.1 (Disaster Recovery Journal 2015) PDFducuhNo ratings yet
- Diabetes Mellitus and Oral Health: An Interprofessional ApproachFrom EverandDiabetes Mellitus and Oral Health: An Interprofessional ApproachNo ratings yet
- Discover Natural -Alternative Therapies for Managing Type 2 DiabetesFrom EverandDiscover Natural -Alternative Therapies for Managing Type 2 DiabetesNo ratings yet
- Operational Readiness Guide - 2017Document36 pagesOperational Readiness Guide - 2017albertocm18100% (2)
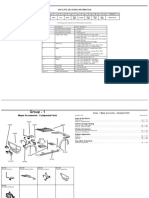
- Hyundai 14 - 16 - 20 - 25BRJ-9Document8 pagesHyundai 14 - 16 - 20 - 25BRJ-9NayanajithNo ratings yet
- Hyperglycaemic EmergenciesDocument11 pagesHyperglycaemic EmergenciesdramaysinghNo ratings yet
- Critical issues in endocrinology and metabolismDocument24 pagesCritical issues in endocrinology and metabolismJorgeNo ratings yet
- Hyperglycemic Emergency in ChildDocument19 pagesHyperglycemic Emergency in ChildSyed Shahrul Naz SyedNo ratings yet
- Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic Syndrome: Review of Acute Decompensated Diabetes in Adult PatientsDocument15 pagesDiabetic Ketoacidosis and Hyperosmolar Hyperglycemic Syndrome: Review of Acute Decompensated Diabetes in Adult PatientsReinaldo MarchenaNo ratings yet
- Diabetic Ketoacidosis and Hyperosmolar. BMJ 2019 PDFDocument15 pagesDiabetic Ketoacidosis and Hyperosmolar. BMJ 2019 PDFJavier Marcano100% (1)
- Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic Syndrome - Review of Acute Decompensated Diabetes in Adult Patients BMJ 2019Document15 pagesDiabetic Ketoacidosis and Hyperosmolar Hyperglycemic Syndrome - Review of Acute Decompensated Diabetes in Adult Patients BMJ 2019capistranflorespalomaNo ratings yet
- Hyperglycemic CrisisDocument9 pagesHyperglycemic CrisisRoberto López MataNo ratings yet
- Diabetic Ketoacidosis and Hyperosmolar Hyperglicemic Syndrome - Review BMJDocument15 pagesDiabetic Ketoacidosis and Hyperosmolar Hyperglicemic Syndrome - Review BMJJorge Flores GonzálezNo ratings yet
- DiabetekDocument15 pagesDiabetekMaira GonzálezNo ratings yet
- Revision Cetoacidosis DiabeticaDocument15 pagesRevision Cetoacidosis DiabeticaChristianNo ratings yet
- _Emergencias Diabeticas BMJ2019 StateDocument15 pages_Emergencias Diabeticas BMJ2019 StateRodrigoNo ratings yet
- 4hyperosmolar Hyperglycemic State (HHS)Document121 pages4hyperosmolar Hyperglycemic State (HHS)desy f sarahNo ratings yet
- PracticalDocument14 pagesPracticalYolanda Arlita AnastasiaNo ratings yet
- Estado Hiperosmolar Hiperglicemico INDocument13 pagesEstado Hiperosmolar Hiperglicemico INbboyhelyNo ratings yet
- Management of Diabetic Ketoacidosis.4Document7 pagesManagement of Diabetic Ketoacidosis.4boomNo ratings yet
- Oajbs Id 000530Document8 pagesOajbs Id 000530Aldy RanggaNo ratings yet
- ZDC 01206002739Document10 pagesZDC 01206002739adi tiarmanNo ratings yet
- Cetoacidosis y Edo Hiperglicemico HiperO 2013Document19 pagesCetoacidosis y Edo Hiperglicemico HiperO 2013RosolinaNo ratings yet
- Management of Diabetic Ketoacidosis in Adults - A Narrative ReviewDocument12 pagesManagement of Diabetic Ketoacidosis in Adults - A Narrative Reviewghr9cjy5npNo ratings yet
- DME-40-0Document12 pagesDME-40-0gdewan364No ratings yet
- Guideline ADA 2010 in Hyperglicemia CrisisDocument9 pagesGuideline ADA 2010 in Hyperglicemia CrisisAissyiyah Nur An NisaNo ratings yet
- Diagnostico y Tratamiento HiperglucemiaDocument16 pagesDiagnostico y Tratamiento HiperglucemiaAndrea Stefania Maldonado MedinaNo ratings yet
- AJGP 05 2019 Focus Willix Hyperglycaemic Presentations WEBDocument5 pagesAJGP 05 2019 Focus Willix Hyperglycaemic Presentations WEBmystatNo ratings yet
- Dia Care 2009 Kitabchi 1335 43crisis HiperglicemicasDocument9 pagesDia Care 2009 Kitabchi 1335 43crisis HiperglicemicassstdocNo ratings yet
- Manage Hyperglycemic CrisesDocument9 pagesManage Hyperglycemic CrisesChristian SalimNo ratings yet
- Diagnosis and management of hyperglycemic crisesDocument13 pagesDiagnosis and management of hyperglycemic crisesTasya SylviaNo ratings yet
- Hyperglycemic Crises in Adult PatientsDocument9 pagesHyperglycemic Crises in Adult PatientslauraNo ratings yet
- Diabetic Medicine - 2022 - Mustafa - Management of Hyperosmolar Hyperglycaemic State HHS in Adults An Updated GuidelineDocument12 pagesDiabetic Medicine - 2022 - Mustafa - Management of Hyperosmolar Hyperglycaemic State HHS in Adults An Updated GuidelineGiancarlo SanteNo ratings yet
- Diabeticketoacidosisand Hyperglycemichyperosmolar State: Jelena Maletkovic,, Andrew DrexlerDocument19 pagesDiabeticketoacidosisand Hyperglycemichyperosmolar State: Jelena Maletkovic,, Andrew DrexlerSiddhartha PalaciosNo ratings yet
- Manejo de Coma Hipermosmolar HHODocument12 pagesManejo de Coma Hipermosmolar HHOCristian Daniel Espinoza ValdezNo ratings yet
- Hyperosmolar Hyperglycemic State (HHS) : Rahayu Oktaliani Aywar ZamriDocument6 pagesHyperosmolar Hyperglycemic State (HHS) : Rahayu Oktaliani Aywar ZamriTrisnaNinaNo ratings yet
- Clinical features, evaluation, and diagnosis of diabetic ketoacidosis and hyperosmolar hyperglycemic stateDocument17 pagesClinical features, evaluation, and diagnosis of diabetic ketoacidosis and hyperosmolar hyperglycemic statejoseaugustorojas9414No ratings yet
- Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in Adults Clinical Features, Evaluation, and DiagnosisDocument17 pagesDiabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in Adults Clinical Features, Evaluation, and DiagnosisAhraxazel Galicia ReynaNo ratings yet
- Second Less Tumor OkDocument19 pagesSecond Less Tumor OkPaolo Mendoza LeonNo ratings yet
- Dmso 7 255 PDFDocument10 pagesDmso 7 255 PDFHening Tirta KusumawardaniNo ratings yet
- Hyperosmolar Hyperglycemic StateDocument8 pagesHyperosmolar Hyperglycemic StateEsra AljafferNo ratings yet
- Complicaciones en DiabetesDocument10 pagesComplicaciones en DiabetesJhaann Franco UPNo ratings yet
- DKA ManagementDocument7 pagesDKA ManagementbababrijeshNo ratings yet
- Medical Clinics of North America Volume 101 Issue 3 2017 (Doi 10.1016 - J.mcna.2016.12.011) Fayfman, Maya Pasquel, Francisco J. Umpierrez, Guillermo E. - Management of Hyperglycemic CrisesDocument20 pagesMedical Clinics of North America Volume 101 Issue 3 2017 (Doi 10.1016 - J.mcna.2016.12.011) Fayfman, Maya Pasquel, Francisco J. Umpierrez, Guillermo E. - Management of Hyperglycemic CrisesBlanca Herrera MoralesNo ratings yet
- Cad EhoDocument14 pagesCad EhomariakjaimesNo ratings yet
- Acute Care of Diabetic PatientsDocument9 pagesAcute Care of Diabetic Patientsseun williamsNo ratings yet
- Diabetes Emergencia Umpierrez 2016Document11 pagesDiabetes Emergencia Umpierrez 2016Nathalie GandoNo ratings yet
- Diabetes, hypertension physiopathology mechanismsDocument7 pagesDiabetes, hypertension physiopathology mechanismschandra9000No ratings yet
- Diabetic Ketoacidosis PDFDocument11 pagesDiabetic Ketoacidosis PDFCsr ArsNo ratings yet
- Hyperglycemic Crises in Adult Patients With DiabetesDocument49 pagesHyperglycemic Crises in Adult Patients With DiabetesrambuNo ratings yet
- 2017 Estado Hiperosmolar Hiperglucemico - 392471761Document8 pages2017 Estado Hiperosmolar Hiperglucemico - 392471761FABIOLA100% (1)
- 75 613 1 PBDocument5 pages75 613 1 PBTowhidulIslamNo ratings yet
- Hyperosmolar Hyperglycemic State (HHS) : Rahayu Oktaliani Aywar ZamriDocument6 pagesHyperosmolar Hyperglycemic State (HHS) : Rahayu Oktaliani Aywar Zamrirsud curupNo ratings yet
- 1 s2.0 S001150292200102X MainDocument17 pages1 s2.0 S001150292200102X MainMabre CazuNo ratings yet
- Nihms 1840957Document35 pagesNihms 1840957Melda AngleNo ratings yet
- Emergency Med Clin N Am Hyperglycemic StateDocument20 pagesEmergency Med Clin N Am Hyperglycemic StateilgarciaNo ratings yet
- Hypoglycemia in DiabetesDocument12 pagesHypoglycemia in Diabetesnaili mumtazatiNo ratings yet
- Hyperglycemic Crise1Document146 pagesHyperglycemic Crise1Vincent ReyesNo ratings yet
- Discover The Best Exercises For Overall Health & Longevity - Based On The Teachings Of Dr. Andrew Huberman: The Ultimate Workout Guide For Lifelong Well-BeingFrom EverandDiscover The Best Exercises For Overall Health & Longevity - Based On The Teachings Of Dr. Andrew Huberman: The Ultimate Workout Guide For Lifelong Well-BeingNo ratings yet
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionFrom EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionNo ratings yet
- Journal Pre-Proofs: Journal of Advanced ResearchDocument55 pagesJournal Pre-Proofs: Journal of Advanced Researchnia rahayu wNo ratings yet
- Journal Pre-Proofs: Cobacter PyloriDocument52 pagesJournal Pre-Proofs: Cobacter Pylorinia rahayu wNo ratings yet
- Journal Pre-Proofs: Cobacter PyloriDocument52 pagesJournal Pre-Proofs: Cobacter Pylorinia rahayu wNo ratings yet
- Journal Pre-Proofs: Journal of Advanced ResearchDocument22 pagesJournal Pre-Proofs: Journal of Advanced Researchnia rahayu wNo ratings yet
- Hearttransplant PDF CarbohydratecountingDocument4 pagesHearttransplant PDF Carbohydratecountingnia rahayu wNo ratings yet
- Dietary Carbohydrates For Diabetics: Current Atherosclerosis Reports July 2012Document8 pagesDietary Carbohydrates For Diabetics: Current Atherosclerosis Reports July 2012nia rahayu wNo ratings yet
- 2007 Pharmacy Times Inpatientglucosecontrol Szumita Greenwood Anger PendergrassDocument12 pages2007 Pharmacy Times Inpatientglucosecontrol Szumita Greenwood Anger Pendergrassnia rahayu wNo ratings yet
- Automatic Determination of Oxidation Number On inDocument8 pagesAutomatic Determination of Oxidation Number On innia rahayu wNo ratings yet
- The Past and Future of The Periodic Table: American Scientist January 2008Document9 pagesThe Past and Future of The Periodic Table: American Scientist January 2008nia rahayu wNo ratings yet
- TN Govt RecruitmentDocument12 pagesTN Govt RecruitmentPriyanka ShankarNo ratings yet
- Dreamers Chords by Jungkook (정국) tabs at Ultimate Guitar ArchiveDocument4 pagesDreamers Chords by Jungkook (정국) tabs at Ultimate Guitar ArchiveLauraNo ratings yet
- Introduction To Human Anatomy & Physiology: Prepared by Mr. Abhay Shripad Joshi Yash Institute of Pharmacy AurangabadDocument18 pagesIntroduction To Human Anatomy & Physiology: Prepared by Mr. Abhay Shripad Joshi Yash Institute of Pharmacy AurangabadMourian AmanNo ratings yet
- IEEE802.11b/g High Power Wireless AP/Bridge Quick Start GuideDocument59 pagesIEEE802.11b/g High Power Wireless AP/Bridge Quick Start GuideonehotminuteNo ratings yet
- Timesheet 25Document1 pageTimesheet 25Gwenzieh TugadeNo ratings yet
- The Essential Guide To Data in The Cloud:: A Handbook For DbasDocument20 pagesThe Essential Guide To Data in The Cloud:: A Handbook For DbasInes PlantakNo ratings yet
- Electrical Experimenter 1915-08Document1 pageElectrical Experimenter 1915-08GNo ratings yet
- Since 1977 Bonds Payable SolutionsDocument3 pagesSince 1977 Bonds Payable SolutionsNah HamzaNo ratings yet
- ISO-14001-2015 EMS RequirementsDocument17 pagesISO-14001-2015 EMS Requirementscuteboom1122No ratings yet
- BS 01726-2-2002Document18 pagesBS 01726-2-2002Joana Casta100% (1)
- List of Candidates for BUDI Scholarship 2016Document9 pagesList of Candidates for BUDI Scholarship 2016Andriawan Mora Anggi HarahapNo ratings yet
- Microsoft Security Product Roadmap Brief All Invitations-2023 AprilDocument5 pagesMicrosoft Security Product Roadmap Brief All Invitations-2023 Apriltsai wen yenNo ratings yet
- Consumer PerceptionDocument61 pagesConsumer PerceptionPrakhar DwivediNo ratings yet
- Transferring Maps To Your Mobile Device (Avenza PDF Maps) : For Apple Products (Ipad, Iphone, Ios)Document2 pagesTransferring Maps To Your Mobile Device (Avenza PDF Maps) : For Apple Products (Ipad, Iphone, Ios)m.naufal nurrahmanNo ratings yet
- Cambridge IGCSE: Combined Science 0653/41Document24 pagesCambridge IGCSE: Combined Science 0653/41jesslynaureliaNo ratings yet
- P150EDocument4 pagesP150EMauro L. KieferNo ratings yet
- Workbook. Unit 3. Exercises 5 To 9. RESPUESTASDocument3 pagesWorkbook. Unit 3. Exercises 5 To 9. RESPUESTASRosani GeraldoNo ratings yet
- SAP HCM - Default Wage Types - Info Type 0008Document6 pagesSAP HCM - Default Wage Types - Info Type 0008cjherrera2No ratings yet
- FINANCIAL REPORTSDocument34 pagesFINANCIAL REPORTSToni111123No ratings yet
- TC-21FJ30LA: Service ManualDocument33 pagesTC-21FJ30LA: Service ManualRajo Peto alamNo ratings yet
- (Leon 2021) Pengaruh Financial Distress, Laverage Terhadap Konservatisme Akuntansi Pada Perusahaan Manfaktur Sektor Konsumsi 2016-2019Document24 pages(Leon 2021) Pengaruh Financial Distress, Laverage Terhadap Konservatisme Akuntansi Pada Perusahaan Manfaktur Sektor Konsumsi 2016-2019PUTRI AYU HASTUTINo ratings yet
- OSK Ekonomi 2016 - SoalDocument19 pagesOSK Ekonomi 2016 - SoalputeNo ratings yet
- Difference between Especially and SpeciallyDocument2 pagesDifference between Especially and SpeciallyCarlos ValenteNo ratings yet