You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- DirtyUSMLE RocksDocument412 pagesDirtyUSMLE RocksDavid S. Chou90% (30)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Effectiveness of Rose Petals and Guava Leaves Extract As A SoapDocument72 pagesThe Effectiveness of Rose Petals and Guava Leaves Extract As A SoapKathy Damaulao80% (5)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Clinical Nursing Skills and Techniques 6th Edition Perry Test BankDocument11 pagesClinical Nursing Skills and Techniques 6th Edition Perry Test BankAnnetteOliverrbwcx100% (12)
- Imp Questions in PharmacologyDocument5 pagesImp Questions in PharmacologyBeerasandrapalyaRangaiahRavikumar100% (3)
- Anesthesia MnemonicsDocument9 pagesAnesthesia MnemonicsLillie Manon100% (1)
- 2016 OITE Study Guide For ResidentsDocument273 pages2016 OITE Study Guide For Residentschu_chiang_3100% (1)
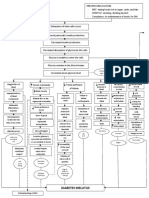
- Diabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)Document3 pagesDiabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)John Henry ValenciaNo ratings yet
- The Final FRCA Short Answer Questions - A Practical Study Guide (PDFDrive)Document348 pagesThe Final FRCA Short Answer Questions - A Practical Study Guide (PDFDrive)Andreea0% (1)
- Goulds Pathophysiology For The Health Professions 6th Edition Vanmeter Test BankDocument8 pagesGoulds Pathophysiology For The Health Professions 6th Edition Vanmeter Test BankJessicaHardysrbxd100% (11)
- 4a's LESSON PLAN FOR GRADE 8 - HealthDocument2 pages4a's LESSON PLAN FOR GRADE 8 - HealthDremie Works100% (1)
- Microbiology - Bio LibretextDocument782 pagesMicrobiology - Bio LibretextJomsEve Ison100% (2)
- Vocabulary Success C1 - SAMPLE PAGES PDFDocument17 pagesVocabulary Success C1 - SAMPLE PAGES PDFAndreas Badeiro100% (1)
- Dex in in Vivo Murine Traumatic Brain Injury ModelDocument5 pagesDex in in Vivo Murine Traumatic Brain Injury ModelSofyan HarahapNo ratings yet
- Dex For Awake Craniotomy Without Laryngeal MaskDocument3 pagesDex For Awake Craniotomy Without Laryngeal MaskSofyan HarahapNo ratings yet
- Searching The Evidence On The Internet: Sudigdo SastroasmoroDocument43 pagesSearching The Evidence On The Internet: Sudigdo SastroasmoroSofyan HarahapNo ratings yet
- EBM and EconomicsDocument14 pagesEBM and EconomicsSofyan HarahapNo ratings yet
- 1ero Bachillerato Semana 3 y 4 Engish 2020-2021Document2 pages1ero Bachillerato Semana 3 y 4 Engish 2020-2021Andres Andy MamallactaNo ratings yet
- Set A: NP1 Nursing Board Exam December 2006 Answer Key 'Foundation of Professional Nursing PracticeDocument14 pagesSet A: NP1 Nursing Board Exam December 2006 Answer Key 'Foundation of Professional Nursing PracticeRaLph C. LopezNo ratings yet
- Rehabilitasi AGA AGBDocument47 pagesRehabilitasi AGA AGBdeasyNo ratings yet
- ICU Related MCQ QuizDocument12 pagesICU Related MCQ Quizezzat salemNo ratings yet
- Cholera Philippine Setting.Document1 pageCholera Philippine Setting.Lara TechiesNo ratings yet
- WPC AssignmentDocument2 pagesWPC AssignmentPragya SinghNo ratings yet
- Fundamentals of Nursing PDocument31 pagesFundamentals of Nursing Papi-26587879100% (4)
- Passive Somking: G Hrithik Roger Kumar Reg No 20BLB1089Document12 pagesPassive Somking: G Hrithik Roger Kumar Reg No 20BLB1089Sathyanarayanan KalyanasundaramNo ratings yet
- New blanki eng ქირურგიის გამოცდაDocument12 pagesNew blanki eng ქირურგიის გამოცდაHarsh NimavatNo ratings yet
- Concept Map Worksheet Olivia Jones Jasgou1752Document2 pagesConcept Map Worksheet Olivia Jones Jasgou1752Jasmyn Rose100% (1)
- Gcse Mock TestsDocument5 pagesGcse Mock TestsTrung Tran VanNo ratings yet
- Abnormal Psychology: Historical and Modern Perspectives: Total Assessment Guide (T.A.G.)Document29 pagesAbnormal Psychology: Historical and Modern Perspectives: Total Assessment Guide (T.A.G.)Rachelle SalcedoNo ratings yet
- 100 Item MEDICAL SURGICAL Nursing Examination Correct Answers and RationalesDocument27 pages100 Item MEDICAL SURGICAL Nursing Examination Correct Answers and RationaleshezekiahNo ratings yet
- Central Dogma and Genetic MedicineDocument4 pagesCentral Dogma and Genetic MedicineedricNo ratings yet
- Medicine Ophthalmology Slide14Document4 pagesMedicine Ophthalmology Slide14testNo ratings yet
- FPF LE01 ContenidosDocument17 pagesFPF LE01 ContenidosBethy Gabriela BriceñoNo ratings yet
- Chapter E132 - Coronavirus Disease (COVID-19)Document31 pagesChapter E132 - Coronavirus Disease (COVID-19)AnasM.GhannoumNo ratings yet
- Medical Management: Medical and Surgical Management of Acute Myocardial InfarctionDocument4 pagesMedical Management: Medical and Surgical Management of Acute Myocardial InfarctionLouie ParillaNo ratings yet