You might also like
- Scars & Devices in Paces 4th Edition PDFDocument132 pagesScars & Devices in Paces 4th Edition PDFKaleem Ullah Bhatti100% (2)
- Robotic Hernia Surgery: A Comprehensive Illustrated GuideFrom EverandRobotic Hernia Surgery: A Comprehensive Illustrated GuideOmar Yusef KudsiNo ratings yet
- 2019-10-16 CPT CodesDocument84 pages2019-10-16 CPT Codesapi-481700794No ratings yet
- Breast Reconstruction After Bilateral ProphylacticDocument9 pagesBreast Reconstruction After Bilateral ProphylacticDirk BucknerNo ratings yet
- Gougoutas 2016Document2 pagesGougoutas 2016salyouhaNo ratings yet
- Postoperative Outcomes of Breast Reconstruction AfDocument6 pagesPostoperative Outcomes of Breast Reconstruction AfDiana AlexandraNo ratings yet
- Oncologic Safety of Conservative Mastectomy in The Therapeutic SettingDocument10 pagesOncologic Safety of Conservative Mastectomy in The Therapeutic SettingIdaamsiyatiNo ratings yet
- BreastReconstruction Review 2016Document9 pagesBreastReconstruction Review 2016Mohammed FaragNo ratings yet
- Breast reconstruction techniques and timingDocument8 pagesBreast reconstruction techniques and timingdiegotequilaNo ratings yet
- 2 StageprepecDocument10 pages2 StageprepecsalyouhaNo ratings yet
- Oncoplastic and Reconstructive BreastDocument14 pagesOncoplastic and Reconstructive BreastYefry Onil Santana Marte100% (1)
- 03 AnatomyDocument9 pages03 AnatomymaytorenacgerNo ratings yet
- Anatomically Based Breast Augmentation: A 6-Plane Autologous ApproachDocument2 pagesAnatomically Based Breast Augmentation: A 6-Plane Autologous Approachcusom34No ratings yet
- Nottingham Approach to Therapeutic Mammoplasty Improves Cosmetic OutcomesDocument13 pagesNottingham Approach to Therapeutic Mammoplasty Improves Cosmetic OutcomesimtinanNo ratings yet
- Chen 2011 Chapter Oncoplastic Techniques For BreastDocument10 pagesChen 2011 Chapter Oncoplastic Techniques For BreastJohn TusselNo ratings yet
- 14 Central Quadrant TechniqueDocument10 pages14 Central Quadrant TechniquemaytorenacgerNo ratings yet
- OncoplasticDocument14 pagesOncoplasticYefry Onil Santana MarteNo ratings yet
- Gox 8 E2578Document12 pagesGox 8 E2578Ade Triansyah EmsilNo ratings yet
- 10.1007@s12609 019 0305 3Document8 pages10.1007@s12609 019 0305 3Yefry Onil Santana MarteNo ratings yet
- Pallarda Et Al. 2019Document4 pagesPallarda Et Al. 2019Walid SasiNo ratings yet
- Kopkash 2018Document6 pagesKopkash 2018Yefry Onil Santana MarteNo ratings yet
- December 2017 1512132618 151Document3 pagesDecember 2017 1512132618 151D Tariq HNo ratings yet
- Revision in Autologous Breast ReconstructionDocument24 pagesRevision in Autologous Breast ReconstructionJose Mauricio Suarez BecerraNo ratings yet
- Pi Is 0002937814024491Document1 pagePi Is 0002937814024491Althaf FathanNo ratings yet
- Managing Complications in AbdominoplastyDocument12 pagesManaging Complications in AbdominoplastyAmanda DaltroNo ratings yet
- Breast Reconstr 2Document15 pagesBreast Reconstr 2Machek AndradaNo ratings yet
- Breast AugmentationDocument12 pagesBreast AugmentationDavid MayoNo ratings yet
- Chun 2011Document6 pagesChun 2011Radityo Budi LeksonoNo ratings yet
- Outcomes of Total Skin-sparing Mastectomy and Immediate ReconstructionDocument8 pagesOutcomes of Total Skin-sparing Mastectomy and Immediate ReconstructionAndreea PopescuNo ratings yet
- Clough K Oncoplasty BJSDocument7 pagesClough K Oncoplasty BJSkomlanihou_890233161No ratings yet
- Sili Kono MaDocument4 pagesSili Kono MaDella Rahmaniar AmelindaNo ratings yet
- ASCO 2014 CrossDocument6 pagesASCO 2014 Crossdrrajeshb77No ratings yet
- Palliative Mastectomy Revisited - PMCDocument4 pagesPalliative Mastectomy Revisited - PMCTony YongNo ratings yet
- 1 s2.0 S174868151730181X MainDocument9 pages1 s2.0 S174868151730181X MainChiara BoccalettoNo ratings yet
- Review: Benjamin O Anderson, Riccardo Masetti, Melvin J SilversteinDocument13 pagesReview: Benjamin O Anderson, Riccardo Masetti, Melvin J SilversteinsanineseinNo ratings yet
- Journal of Surgical Oncology - 2013 - Fortunato - When Mastectomy Is Needed Is The Nipple Sparing Procedure A New StandardDocument6 pagesJournal of Surgical Oncology - 2013 - Fortunato - When Mastectomy Is Needed Is The Nipple Sparing Procedure A New StandardJethro ConcepcionNo ratings yet
- S. A. Robertson., 2014Document13 pagesS. A. Robertson., 2014ajeng hefdeaNo ratings yet
- Letter A incision periareolar mastopexy with breast implant augmentation-dr. kamal hussein saleh-consultant cosmetic surgeon-al emadi hospital-qatar-doha,زرق ابر البوتوكس,جراحة التجميل,تجميل الانف,تجميل الثدي,تكبير الثدي,تكبير الارداف,مستشفى العمادي,قطر,دبيDocument5 pagesLetter A incision periareolar mastopexy with breast implant augmentation-dr. kamal hussein saleh-consultant cosmetic surgeon-al emadi hospital-qatar-doha,زرق ابر البوتوكس,جراحة التجميل,تجميل الانف,تجميل الثدي,تكبير الثدي,تكبير الارداف,مستشفى العمادي,قطر,دبيDR. KAMAL HUSSEIN SALEH AL HUSSEINY100% (1)
- Alloderm - Breast ReconstructionDocument180 pagesAlloderm - Breast ReconstructionFlorina PopaNo ratings yet
- The Effect of Biological Scaffold (Biodesign) in Postmastectomy Direct-to-Implant Breast ReconstructionDocument7 pagesThe Effect of Biological Scaffold (Biodesign) in Postmastectomy Direct-to-Implant Breast Reconstruction郭竹瑩No ratings yet
- Prot SAP 000 PDFDocument11 pagesProt SAP 000 PDFdrrajeshb77No ratings yet
- Sciencedirect: Improving Outcomes in Breast Reconstruction: From Implant-Based Techniques Towards Tissue RegenerationDocument5 pagesSciencedirect: Improving Outcomes in Breast Reconstruction: From Implant-Based Techniques Towards Tissue RegenerationRita DiabNo ratings yet
- Flap ReconstructionDocument7 pagesFlap ReconstructionATUL178No ratings yet
- Weber 2020Document11 pagesWeber 2020Yefry Onil Santana MarteNo ratings yet
- TULUA Springer PDFDocument10 pagesTULUA Springer PDFCésar Cuadros SerranoNo ratings yet
- New Trends in Breast Cancer Surgery: A Therapeutic Approach Increasingly Efficacy and Respectful of The PatientDocument8 pagesNew Trends in Breast Cancer Surgery: A Therapeutic Approach Increasingly Efficacy and Respectful of The PatientleonardoNo ratings yet
- Partial Mastectomy ReconstructionDocument12 pagesPartial Mastectomy ReconstructionJose Mauricio Suarez BecerraNo ratings yet
- Annals of Medicine and Surgery: M. Riis TDocument13 pagesAnnals of Medicine and Surgery: M. Riis TJacob AlajyNo ratings yet
- Breast Reconstruction After Mastectomy For Breast Tumor: About 24 CasesDocument6 pagesBreast Reconstruction After Mastectomy For Breast Tumor: About 24 CasesIJAR JOURNALNo ratings yet
- Clinical Study: Extreme Oncoplastic Surgery For Multifocal/Multicentric and Locally Advanced Breast CancerDocument9 pagesClinical Study: Extreme Oncoplastic Surgery For Multifocal/Multicentric and Locally Advanced Breast CancerAsti DwiningsihNo ratings yet
- Jurnal Breast Rekon Presentasi 10 Okt 18 RevisiDocument57 pagesJurnal Breast Rekon Presentasi 10 Okt 18 RevisiFebriadi RNo ratings yet
- Critch Ley 2016Document11 pagesCritch Ley 2016leonardo100% (1)
- INCISION PATTERNS IN BREAST ONCOPLASTIC SURGERYDocument26 pagesINCISION PATTERNS IN BREAST ONCOPLASTIC SURGERYccmcshh surgeryNo ratings yet
- Unukovych 2016Document7 pagesUnukovych 2016jdavies231No ratings yet
- Asian GynecomastiaDocument5 pagesAsian GynecomastiaAngga Putra Kusuma KusumaNo ratings yet
- Quilting Sutures Reduces Seroma in Mastectomy: Original StudyDocument5 pagesQuilting Sutures Reduces Seroma in Mastectomy: Original StudydickyNo ratings yet
- Nihms 1653808Document16 pagesNihms 1653808luis david gomez gonzalezNo ratings yet
- Overview of Current Trends in Hysterectomy: ReviewDocument13 pagesOverview of Current Trends in Hysterectomy: ReviewFranklin Salirrosas CernaNo ratings yet
- ArticuloDocument6 pagesArticuloadrianarocio57No ratings yet
- Jurnal Hernia VentralisDocument10 pagesJurnal Hernia VentralisMusdalipaNo ratings yet
- Elkhoury 2015Document5 pagesElkhoury 2015mod_naiveNo ratings yet
- Oncoplastic Breast Surgery Techniques for the General SurgeonFrom EverandOncoplastic Breast Surgery Techniques for the General SurgeonNo ratings yet
- Preoperative Imaging in Staghorn Calculi, Planning and Decision Making in Management of Staghorn CalculiDocument7 pagesPreoperative Imaging in Staghorn Calculi, Planning and Decision Making in Management of Staghorn CalculiBenny KurniawanNo ratings yet
- The Role of Benign Prostatic Hyperplasia Treatments in Ejaculatory DysfunctionDocument7 pagesThe Role of Benign Prostatic Hyperplasia Treatments in Ejaculatory DysfunctionJuwita Dewi PratiwiNo ratings yet
- Marek 2014Document6 pagesMarek 2014Juwita Dewi PratiwiNo ratings yet
- Data Trauma Ginjal Pediatric Makassar 2014-2018 NewDocument4 pagesData Trauma Ginjal Pediatric Makassar 2014-2018 NewJuwita Dewi PratiwiNo ratings yet
- How Ethics Failed - The Role of Psychiatrists and Physicians in Nazi Programs From Exclusion To Extermination, 1933-1945Document28 pagesHow Ethics Failed - The Role of Psychiatrists and Physicians in Nazi Programs From Exclusion To Extermination, 1933-1945Juwita Dewi PratiwiNo ratings yet
- Data Trauma Ginjal Pediatric Makassar 2014-2018 NewDocument4 pagesData Trauma Ginjal Pediatric Makassar 2014-2018 NewJuwita Dewi PratiwiNo ratings yet
- Institutional Review Board IRB and Ethical Issues - AnnotatedDocument11 pagesInstitutional Review Board IRB and Ethical Issues - AnnotatedJuwita Dewi PratiwiNo ratings yet
- Lower Urinary Tract Symptoms Associated With DJ StentDocument7 pagesLower Urinary Tract Symptoms Associated With DJ StentJuwita Dewi PratiwiNo ratings yet
- Operan Jaga Igd 17 Desember 2020Document2 pagesOperan Jaga Igd 17 Desember 2020Juwita Dewi PratiwiNo ratings yet
- Poster Abstracts 1Document16 pagesPoster Abstracts 1Juwita Dewi PratiwiNo ratings yet
- GREETINGSDocument1 pageGREETINGSJuwita Dewi PratiwiNo ratings yet
- Oesophageal Cancer - Case Report and Literature ReviewDocument4 pagesOesophageal Cancer - Case Report and Literature ReviewJuwita Dewi PratiwiNo ratings yet
- Operan Jaga 11 Nov 20Document1 pageOperan Jaga 11 Nov 20Juwita Dewi PratiwiNo ratings yet
- Lembar Penilaian OPDocument1 pageLembar Penilaian OPJuwita Dewi PratiwiNo ratings yet
- Operan Pasien Igd Bedah, Senin 2 November 2020: DR - Dr.ronald E.Lusikooy, SP.B-KBDDocument1 pageOperan Pasien Igd Bedah, Senin 2 November 2020: DR - Dr.ronald E.Lusikooy, SP.B-KBDJuwita Dewi PratiwiNo ratings yet
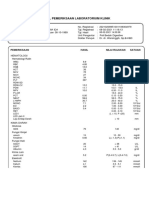
- Hasil Pemeriksaan Laboratorium KlinikDocument2 pagesHasil Pemeriksaan Laboratorium KlinikJuwita Dewi PratiwiNo ratings yet
- GREETINGSDocument1 pageGREETINGSJuwita Dewi PratiwiNo ratings yet
- 5 6091205456221438340 PDFDocument1 page5 6091205456221438340 PDFJuwita Dewi PratiwiNo ratings yet
- Breast Reconstruction: Rekonstrukcija DojkeDocument7 pagesBreast Reconstruction: Rekonstrukcija DojkeJuwita Dewi PratiwiNo ratings yet
- TRAM (Transverse Rectus Abdominis Muscle) Flap: Pedicled Muscle or Musculocutaneous FlapsDocument7 pagesTRAM (Transverse Rectus Abdominis Muscle) Flap: Pedicled Muscle or Musculocutaneous FlapsJuwita Dewi PratiwiNo ratings yet
- Principles of Bariatric and Metabolic SurgeryDocument51 pagesPrinciples of Bariatric and Metabolic SurgeryDr Shahzad Alam ShahNo ratings yet
- Principles of Minimal Invasive SurgeryDocument39 pagesPrinciples of Minimal Invasive SurgeryAvinash KannanNo ratings yet
- Preservation Rhinoplasty: Plastic and Reconstructive Surgery - February 2020Document1 pagePreservation Rhinoplasty: Plastic and Reconstructive Surgery - February 2020enviNo ratings yet
- Steinmann PinDocument3 pagesSteinmann Pinrachelmores12No ratings yet
- Umesh Singh. TLTK-47Document5 pagesUmesh Singh. TLTK-47HẢI HOÀNG THANHNo ratings yet
- Data Age.Document66 pagesData Age.Kamal GpNo ratings yet
- PHTY205 2023 W10 L1 Cardiothoracic SurgeryDocument18 pagesPHTY205 2023 W10 L1 Cardiothoracic SurgerynaveennaguleswaranNo ratings yet
- Tindakan Mata Icd 9 CMDocument15 pagesTindakan Mata Icd 9 CMrekam medisNo ratings yet
- Ileal Pouches: Chapter 189: Supravesical Urinary DiversionDocument1 pageIleal Pouches: Chapter 189: Supravesical Urinary DiversioncesaliapNo ratings yet
- Chest Tube Insertion GuideDocument8 pagesChest Tube Insertion GuideTaufik Nur YahyaNo ratings yet
- Penggolongan OperasiDocument32 pagesPenggolongan OperasiKARTIKANo ratings yet
- Walthauser H. Viaje, M.D., FpcsDocument1 pageWalthauser H. Viaje, M.D., FpcsRegine EnvidiadoNo ratings yet
- OSRG Assignment DR YehyaDocument5 pagesOSRG Assignment DR YehyaRouba Al hamadNo ratings yet
- AbbreviationDocument2 pagesAbbreviationdwlnuestro10No ratings yet
- Temno Biopsy family brochureDocument6 pagesTemno Biopsy family brochureBright HealthNo ratings yet
- Ayushman Packages-Procedures PDFDocument169 pagesAyushman Packages-Procedures PDFAmbuj Kumar SoniNo ratings yet
- Ayushman Bharat General Surgery List 5Document3 pagesAyushman Bharat General Surgery List 5Rahul SakalleNo ratings yet
- Christiaan BarnardDocument3 pagesChristiaan BarnardSlavomíra LaukováNo ratings yet
- Esophageal Resection & Reconstruction TechniquesDocument71 pagesEsophageal Resection & Reconstruction TechniquesFlaviu Ionuț FaurNo ratings yet
- Surgical Suture Materials Are Used in The Closure of Most Wound Types. The Ideal SutureDocument9 pagesSurgical Suture Materials Are Used in The Closure of Most Wound Types. The Ideal SutureToria053No ratings yet
- Hair Transplantation: Current Concepts and Techniques: Walter P. Unger WDocument5 pagesHair Transplantation: Current Concepts and Techniques: Walter P. Unger WAbhishek ChauhanNo ratings yet
- Data Faktur Apotik Mutiara InsaniDocument13 pagesData Faktur Apotik Mutiara Insaniapotek mutiarainsaniNo ratings yet
- Expo de RCP Post QX CardiacaDocument14 pagesExpo de RCP Post QX CardiacaJulia Torres del AguilaNo ratings yet
- Posterior Fixation of Gastric Tube With Fibrin SeaDocument6 pagesPosterior Fixation of Gastric Tube With Fibrin Seaabdourahmane ndongNo ratings yet
- Audit FinalisedDocument346 pagesAudit FinalisednatheNo ratings yet
- Lista de Precios Arthrex Consumibles 2022Document32 pagesLista de Precios Arthrex Consumibles 2022Gerardo OlagueNo ratings yet
- CGHS Rates 2014 - Hyderabad4Document51 pagesCGHS Rates 2014 - Hyderabad4HeliosAlaricNo ratings yet
- Rate ListDocument37 pagesRate ListUsman GhaniNo ratings yet