You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Structural Design Basis ReportDocument31 pagesStructural Design Basis ReportRajaram100% (1)
- Peter Szekeres-Solutions To Problems of A Course in Modern Mathematical Physics - Groups, Hilbert Space and Differential Geometry PDFDocument382 pagesPeter Szekeres-Solutions To Problems of A Course in Modern Mathematical Physics - Groups, Hilbert Space and Differential Geometry PDFMed Chouaybi0% (1)
- Governance Operating Model: Structure Oversight Responsibilities Talent and Culture Infrastructu REDocument6 pagesGovernance Operating Model: Structure Oversight Responsibilities Talent and Culture Infrastructu REBob SolísNo ratings yet
- VOTOL EMController Manual V2.0Document18 pagesVOTOL EMController Manual V2.0Nandi F. ReyhanNo ratings yet
- Quality Standards For ECCE INDIA PDFDocument41 pagesQuality Standards For ECCE INDIA PDFMaryam Ben100% (4)
- Code of Ethics For Civil Engineers PiceDocument3 pagesCode of Ethics For Civil Engineers PiceEdwin Ramos Policarpio100% (3)
- Control ValvesDocument95 pagesControl ValvesHardik Acharya100% (1)
- Ahmed SLE Mcq-P1Document201 pagesAhmed SLE Mcq-P1Mohammed Qasim Al-Watary88% (34)
- Preventive OrthodonticDocument19 pagesPreventive OrthodonticNada EmadNo ratings yet
- Biology of Tooth Movement: Presented By: Nada Emad Elhossiney Supervised byDocument140 pagesBiology of Tooth Movement: Presented By: Nada Emad Elhossiney Supervised byNada EmadNo ratings yet
- Life and Works of Jose Rizal Modified ModuleDocument96 pagesLife and Works of Jose Rizal Modified ModuleRamos, Queencie R.No ratings yet
- Chromatographic TechniquesDocument2 pagesChromatographic TechniquesNada EmadNo ratings yet
- Assessment of The KnowledgeDocument5 pagesAssessment of The KnowledgeNada EmadNo ratings yet
- Facemask in Treatment of classIIIDocument31 pagesFacemask in Treatment of classIIINada EmadNo ratings yet
- Mechanotransduction of Orthodontic ForcesDocument4 pagesMechanotransduction of Orthodontic ForcesNada EmadNo ratings yet
- White Spot Lesions An Iatrogenic Damage After Orthodontic Treatment Its Prevention and Management An Overview 2161 1122.1000123Document3 pagesWhite Spot Lesions An Iatrogenic Damage After Orthodontic Treatment Its Prevention and Management An Overview 2161 1122.1000123Nada EmadNo ratings yet
- Black Stains in Primary Teeth OverviewDocument2 pagesBlack Stains in Primary Teeth OverviewNada EmadNo ratings yet
- Restorative and Pulp Treatment of Primary and Young May 2015Document48 pagesRestorative and Pulp Treatment of Primary and Young May 2015Nada EmadNo ratings yet
- Borges2016white Spot LesionDocument8 pagesBorges2016white Spot LesionNada EmadNo ratings yet
- Class III IV Composite Rest. 1Document30 pagesClass III IV Composite Rest. 1Puteri NazirahNo ratings yet
- Clinical Evaluation of Dental Alignment and LeveliDocument8 pagesClinical Evaluation of Dental Alignment and LeveliNada EmadNo ratings yet
- Crown in Paedatric DentistryDocument6 pagesCrown in Paedatric DentistrySTEFFI MIFTANo ratings yet
- Accuracy of Several Implant Bite Registration TechDocument9 pagesAccuracy of Several Implant Bite Registration TechNada EmadNo ratings yet
- BP Restorativedent PDFDocument13 pagesBP Restorativedent PDFFrancisca AndreaNo ratings yet
- Effects of Three Different Topical Agents On Enamel Demineralization Around Orthodontic Brackets A Clinical StudyDocument4 pagesEffects of Three Different Topical Agents On Enamel Demineralization Around Orthodontic Brackets A Clinical StudyNada EmadNo ratings yet
- CJT 041Document8 pagesCJT 041Nada EmadNo ratings yet
- Dentistry: Bonding Metal Brackets On Tooth SurfacesDocument6 pagesDentistry: Bonding Metal Brackets On Tooth SurfacesNada EmadNo ratings yet
- Article Saods 19 Css 1096Document11 pagesArticle Saods 19 Css 1096Nada EmadNo ratings yet
- Ccide-11-89 SmileDocument13 pagesCcide-11-89 SmileNada EmadNo ratings yet
- 3M - 93C HallTechGuide2191110 PDFDocument21 pages3M - 93C HallTechGuide2191110 PDFDuvan CastilloNo ratings yet
- 038AJO2017 152 116 25 ClIII Latopenbite CrossbiteDocument11 pages038AJO2017 152 116 25 ClIII Latopenbite CrossbiteNada EmadNo ratings yet
- Dentistry: Bonding Metal Brackets On Tooth SurfacesDocument6 pagesDentistry: Bonding Metal Brackets On Tooth SurfacesNada EmadNo ratings yet
- Restorative and Pulp Treatment of Primary and Young May 2015Document48 pagesRestorative and Pulp Treatment of Primary and Young May 2015Nada EmadNo ratings yet
- Serialextraction 2Document6 pagesSerialextraction 2Zullia TaftyantiNo ratings yet
- BP Restorativedent PDFDocument13 pagesBP Restorativedent PDFFrancisca AndreaNo ratings yet
- 3M - 93C HallTechGuide2191110 PDFDocument21 pages3M - 93C HallTechGuide2191110 PDFDuvan CastilloNo ratings yet
- Facemask in Treatment of classIIIDocument31 pagesFacemask in Treatment of classIIINada EmadNo ratings yet
- 53 English Work Book XDocument292 pages53 English Work Book XArun DhawanNo ratings yet
- Bring Your Gear 2010: Safely, Easily and in StyleDocument76 pagesBring Your Gear 2010: Safely, Easily and in StyleAkoumpakoula TampaoulatoumpaNo ratings yet
- Section 1 Company Overview StandardsDocument34 pagesSection 1 Company Overview StandardsChris MedeirosNo ratings yet
- 2.0. Design, Protection and Sizing of Low Voltage Electrical Installations (Wiring) To IEE Wiring Regulations BS 7671 MS IEC (IEC) 60364 - 16&17.12.15Document2 pages2.0. Design, Protection and Sizing of Low Voltage Electrical Installations (Wiring) To IEE Wiring Regulations BS 7671 MS IEC (IEC) 60364 - 16&17.12.15Edison LimNo ratings yet
- Digital Systems Project: IITB CPUDocument7 pagesDigital Systems Project: IITB CPUAnoushka DeyNo ratings yet
- Object Oriented ParadigmDocument2 pagesObject Oriented ParadigmDickson JohnNo ratings yet
- Installation 59TP6A 08SIDocument92 pagesInstallation 59TP6A 08SIHenry SmithNo ratings yet
- BIOAVAILABILITY AND BIOEQUIVALANCE STUDIES Final - PPTX'Document32 pagesBIOAVAILABILITY AND BIOEQUIVALANCE STUDIES Final - PPTX'Md TayfuzzamanNo ratings yet
- Hofstede's Cultural DimensionsDocument35 pagesHofstede's Cultural DimensionsAALIYA NASHATNo ratings yet
- Jinivefsiti: Sultan LorisDocument13 pagesJinivefsiti: Sultan LorisSITI HAJAR BINTI MOHD LATEPINo ratings yet
- Unit 2: Air Intake and Exhaust SystemsDocument10 pagesUnit 2: Air Intake and Exhaust SystemsMahmmod Al-QawasmehNo ratings yet
- Six Sigma PresentationDocument17 pagesSix Sigma PresentationDhular HassanNo ratings yet
- Vetoset CA541: Thickbed Cementitious Tile AdhesiveDocument2 pagesVetoset CA541: Thickbed Cementitious Tile Adhesivemus3b1985No ratings yet
- SCD Course List in Sem 2.2020 (FTF or Online) (Updated 02 July 2020)Document2 pagesSCD Course List in Sem 2.2020 (FTF or Online) (Updated 02 July 2020)Nguyễn Hồng AnhNo ratings yet
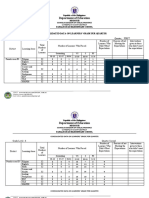
- Department of Education: Consolidated Data On Learners' Grade Per QuarterDocument4 pagesDepartment of Education: Consolidated Data On Learners' Grade Per QuarterUsagi HamadaNo ratings yet
- MLX90614Document44 pagesMLX90614ehsan1985No ratings yet
- DTR Testastretta Valve Adjustment ProcedureDocument10 pagesDTR Testastretta Valve Adjustment ProcedureTony LamprechtNo ratings yet
- Ilovepdf MergedDocument503 pagesIlovepdf MergedHemantNo ratings yet
- FS-1040 FS-1060DN: Parts ListDocument23 pagesFS-1040 FS-1060DN: Parts List1980cvvrNo ratings yet
- RH-A Catalog PDFDocument1 pageRH-A Catalog PDFAchmad KNo ratings yet
- CL Honours Report NamanDocument11 pagesCL Honours Report NamanNaman VermaNo ratings yet
- 147 Amity Avenue Nampa, ID 81937 (999) 999-9999 William at Email - ComDocument4 pages147 Amity Avenue Nampa, ID 81937 (999) 999-9999 William at Email - ComjeyesbelmenNo ratings yet