You might also like
- Science5 - q2 - Mod2 - Menstrual Cycle - v4Document20 pagesScience5 - q2 - Mod2 - Menstrual Cycle - v4Nellen Grace Ortiz86% (7)
- Sanford Knee Injury Prevention ProgramDocument44 pagesSanford Knee Injury Prevention ProgramRichard Van RickleyNo ratings yet
- Company Name Industry Vertical Board Numbaddress City State ZipcodeDocument8 pagesCompany Name Industry Vertical Board Numbaddress City State ZipcodeVaibhav SarateNo ratings yet
- DLL Science 8-4thQ-2Document4 pagesDLL Science 8-4thQ-2anon_298904132100% (3)
- Nursing Leadership and Management Practice TestDocument1 pageNursing Leadership and Management Practice TestMikhaela GonzalesNo ratings yet
- Wou 2021 8march ProjectDocument13 pagesWou 2021 8march ProjectdhilaNo ratings yet
- Global and Indonesian's Update On COVID19Document23 pagesGlobal and Indonesian's Update On COVID19Tasia DeastutiNo ratings yet
- WOU 2021 5apr ClearedDocument13 pagesWOU 2021 5apr CleareddhilaNo ratings yet
- WOU 2021 17may Cleared1Document15 pagesWOU 2021 17may Cleared1Muslim CreativeNo ratings yet
- Wou 9 September 2020 ClearedDocument11 pagesWou 9 September 2020 ClearedMessyAnd InStyleNo ratings yet
- Wou 1february2021Document12 pagesWou 1february2021dhilaNo ratings yet
- Wou 1408 ApprovedDocument13 pagesWou 1408 ApprovedDanilo RosaNo ratings yet
- Philippines Welcomes The Arrival of COVIDDocument10 pagesPhilippines Welcomes The Arrival of COVIDMarjourie Louise BelaiNo ratings yet
- Article: Dealing With Vaccine Hesitancy in Africa: The Prospective COVID-19 Vaccine ContextDocument7 pagesArticle: Dealing With Vaccine Hesitancy in Africa: The Prospective COVID-19 Vaccine ContextA009Karin Kurniati NurfatmahNo ratings yet
- Vaccines 09 00175Document14 pagesVaccines 09 00175Strudwick AyambaNo ratings yet
- PIIS2213260021001296Document2 pagesPIIS2213260021001296fareha riazNo ratings yet
- Lessons Learned and Good Practices Immunization Activities During The COVID 19 Pandemic 2021Document86 pagesLessons Learned and Good Practices Immunization Activities During The COVID 19 Pandemic 2021nejatseid46No ratings yet
- Covax: A Broken Promise To The WorldDocument16 pagesCovax: A Broken Promise To The WorldDavide FalcioniNo ratings yet
- Endoscopy Guidline in Covid 19 EraDocument6 pagesEndoscopy Guidline in Covid 19 EraAmik IndrayaniNo ratings yet
- Wou 28 August ApprovedDocument14 pagesWou 28 August ApprovedMessyAnd InStyleNo ratings yet
- SoongtewubezDocument13 pagesSoongtewubezDooga BeubiezeNo ratings yet
- StaffDocument2 pagesStaffandros 77No ratings yet
- Who Situation Report - May 2022 - Coxs Bazar 5Document3 pagesWho Situation Report - May 2022 - Coxs Bazar 5Michael GamukoNo ratings yet
- WHO Report On COVID-19 - April 22, 2020Document14 pagesWHO Report On COVID-19 - April 22, 2020CityNewsTorontoNo ratings yet
- Advisory 52 FinalDocument1 pageAdvisory 52 FinalCATHERINE HAYNESNo ratings yet
- WHO's Monthly Operational Update On COVID-19Document18 pagesWHO's Monthly Operational Update On COVID-19davidNo ratings yet
- Vaccination Certificate Information: Un System-Wide Covid-19 Vaccination ProgrammeDocument12 pagesVaccination Certificate Information: Un System-Wide Covid-19 Vaccination ProgrammeYusuf HidayatNo ratings yet
- COVID-19 Vaccine Hesitancy in South Africa: How Can We Maximize Uptake of COVID-19 Vaccines?Document14 pagesCOVID-19 Vaccine Hesitancy in South Africa: How Can We Maximize Uptake of COVID-19 Vaccines?A009Karin Kurniati NurfatmahNo ratings yet
- Covid-19 Vaccines: Ethical, Legal and Practical ConsiderationsDocument3 pagesCovid-19 Vaccines: Ethical, Legal and Practical ConsiderationsJohn SutphinNo ratings yet
- Jpha 14 5 2290Document5 pagesJpha 14 5 2290WOYOPWA SHEMNo ratings yet
- UNICEF Guinea COVID-19 Situation Report No. 9 - 27 May To 9 June 2020Document5 pagesUNICEF Guinea COVID-19 Situation Report No. 9 - 27 May To 9 June 2020UNICEFGuineaNo ratings yet
- Corona Pandemic: by Ria Grover Class XB Roll No.36Document6 pagesCorona Pandemic: by Ria Grover Class XB Roll No.36RIA 92462No ratings yet
- 1 s2.0 S1074761321002612 MainDocument10 pages1 s2.0 S1074761321002612 Mainellslister15No ratings yet
- Neonates in The COVID-19 Pandemic: EditorialDocument3 pagesNeonates in The COVID-19 Pandemic: EditorialadeNo ratings yet
- Idr 13 00064Document15 pagesIdr 13 00064Dmytro DemashNo ratings yet
- Sars-Cov-2 A Public Health Emergency: Challenges in Vaccination in Indian SetupDocument5 pagesSars-Cov-2 A Public Health Emergency: Challenges in Vaccination in Indian Setupgaurav pandeyNo ratings yet
- Who CXB Situation Report 29Document8 pagesWho CXB Situation Report 29Zisan AhmedNo ratings yet
- Program Imunisasi COVID-19 Kebangsaan - Ms.enDocument26 pagesProgram Imunisasi COVID-19 Kebangsaan - Ms.enpirekNo ratings yet
- Wou 8february2021 ClearedDocument12 pagesWou 8february2021 CleareddhilaNo ratings yet
- Ghana Fs 2022Document2 pagesGhana Fs 2022John SlorNo ratings yet
- Corona - 15-20Document6 pagesCorona - 15-20amourionresearcherNo ratings yet
- Consensus Interim Recommendations On The Use of Coronavac in HK As of 19 Feb 2021Document6 pagesConsensus Interim Recommendations On The Use of Coronavac in HK As of 19 Feb 2021Felipe Barros S.No ratings yet
- ASTRAZENECA MEDIA STATEMENT - 100 Countries & Counting Have Received Life-Saving COVID-19 Vaccines Via COVAXDocument3 pagesASTRAZENECA MEDIA STATEMENT - 100 Countries & Counting Have Received Life-Saving COVID-19 Vaccines Via COVAXzuco.newsriseNo ratings yet
- WHO 2019 NCoV Vaccination IPC 2021.1 EngDocument4 pagesWHO 2019 NCoV Vaccination IPC 2021.1 EngsusiNo ratings yet
- UNICEF Guinea COVID-19 Situation Report No. 8. As of 26 May 2020Document5 pagesUNICEF Guinea COVID-19 Situation Report No. 8. As of 26 May 2020UNICEFGuineaNo ratings yet
- Clinical Outcomes of A COVID-19 Vaccine: Implementation Over EfficacyDocument19 pagesClinical Outcomes of A COVID-19 Vaccine: Implementation Over EfficacyIraNo ratings yet
- Vaksin 2Document9 pagesVaksin 2Arumm88No ratings yet
- Preprints202104 0702 v1Document13 pagesPreprints202104 0702 v1JicelleNo ratings yet
- Manual Vacunas Covid (059-116)Document58 pagesManual Vacunas Covid (059-116)MONTOYA CABANILLAS RAINIER IVANNo ratings yet
- Preprints202209 0430 v2Document23 pagesPreprints202209 0430 v2rennanfromNo ratings yet
- UNICEF Ghana COVID19 Situation Report No 6 16 30 June 2020Document9 pagesUNICEF Ghana COVID19 Situation Report No 6 16 30 June 2020aigraineNo ratings yet
- Research ProjectDocument12 pagesResearch Projectark borNo ratings yet
- Articles Roncier VIH - ORG IAS 2023Document3 pagesArticles Roncier VIH - ORG IAS 2023r8jbbfw57xNo ratings yet
- COVID-19 Vaccine and Pregnancy A Safety Weapon Against PandemicDocument10 pagesCOVID-19 Vaccine and Pregnancy A Safety Weapon Against Pandemicdr.ulfaluthfianiNo ratings yet
- (DR) ONIMISI Anthony Baba & Isaac Sugar Ray.: RD THDocument4 pages(DR) ONIMISI Anthony Baba & Isaac Sugar Ray.: RD THBrian JollensNo ratings yet
- Human Papillomavirus Vaccine: Supply and Demand UpdateDocument13 pagesHuman Papillomavirus Vaccine: Supply and Demand UpdatelindsayNo ratings yet
- Vaccines 10 00246Document17 pagesVaccines 10 00246john paul carasNo ratings yet
- Final COVID 19 Vaccine Campaign TrainingDocument85 pagesFinal COVID 19 Vaccine Campaign TrainingMfm 2015No ratings yet
- Kingston Gleaner Nov 18 2022 P 38Document1 pageKingston Gleaner Nov 18 2022 P 38whoopsoopsNo ratings yet
- 1 s2.0 S0264410X1930163X MainDocument7 pages1 s2.0 S0264410X1930163X Mainzezo.3kxNo ratings yet
- Philippines: Situation Report 13Document5 pagesPhilippines: Situation Report 13Krizzia Mae Soriano-Sta InesNo ratings yet
- IDS - COVID-19 VaccinationDocument7 pagesIDS - COVID-19 VaccinationRenrenz PayumoNo ratings yet
- Pregnan Women Perseption of Covid 19 VaksinDocument11 pagesPregnan Women Perseption of Covid 19 VaksinLusyi AnnisaNo ratings yet
- BreastfeedingDocument14 pagesBreastfeedingSuad jakalatNo ratings yet
- Project 2: Technical University of DenmarkDocument11 pagesProject 2: Technical University of DenmarkRiyaz AlamNo ratings yet
- Wet My Pantys and Have Pulsating OrgasmDocument1 pageWet My Pantys and Have Pulsating OrgasmIbrahimovic HelenaNo ratings yet
- TU Institute of Medicine Entrance Result 2068Document6 pagesTU Institute of Medicine Entrance Result 2068Dristhi ShresthaNo ratings yet
- WD 3-October ProjectsDocument2 pagesWD 3-October Projectsfake name100% (2)
- The National Academies Press: Risk Assessment of Proposed ARFF Standards (2011)Document105 pagesThe National Academies Press: Risk Assessment of Proposed ARFF Standards (2011)Marius BuysNo ratings yet
- School Policies and Their FunctionDocument11 pagesSchool Policies and Their FunctionJessa Mae PerfiñanNo ratings yet
- Case-Digest-Imbong-V-Ochoa Part 2Document6 pagesCase-Digest-Imbong-V-Ochoa Part 2Kate Hazzle JandaNo ratings yet
- 03.affinity Efficacy PotencyDocument33 pages03.affinity Efficacy PotencyelitechemsNo ratings yet
- Role of The Technician: Lynn Lawrence, CPOT, ABOC, COADocument6 pagesRole of The Technician: Lynn Lawrence, CPOT, ABOC, COASumon SarkarNo ratings yet
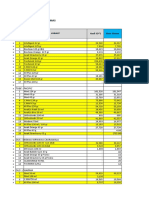
- Bahan Kemas - Selisih SO Vs Sistem FY2020 - 291220Document17 pagesBahan Kemas - Selisih SO Vs Sistem FY2020 - 291220Idan RidwanNo ratings yet
- Las Grade 7Document16 pagesLas Grade 7Badeth Ablao67% (3)
- G9 Learning Module Week 1Document6 pagesG9 Learning Module Week 1Pang ChixxNo ratings yet
- The Bad Weather, He Still Chooses To Go: Soal UASBN Lintas Minat Bahasa InggrisDocument7 pagesThe Bad Weather, He Still Chooses To Go: Soal UASBN Lintas Minat Bahasa InggrisHilwa FitriNo ratings yet
- Ulzii 2020Document12 pagesUlzii 2020Arsyheilla FbrNo ratings yet
- Contract MarysolDocument3 pagesContract MarysolJacqueline Ponce PinosNo ratings yet
- DX by UsgDocument59 pagesDX by UsgJagger JaggerNo ratings yet
- Nursing As A ProfessionDocument9 pagesNursing As A Professionvivian joy bulosanNo ratings yet
- Biology Curriculum and Assessment Guide (Secondary 4 - 6) : Science Education Key Learning AreaDocument139 pagesBiology Curriculum and Assessment Guide (Secondary 4 - 6) : Science Education Key Learning AreaUniversityJC100% (1)
- Journalof Media Psychology 112008Document40 pagesJournalof Media Psychology 112008MUHAMMAD CHAMDAN HUSEINNo ratings yet
- Deogracias - Persuasive SpeechDocument4 pagesDeogracias - Persuasive SpeechJameson DeograciasNo ratings yet
- Unit of Competency: Practice Occupational Health and Safety Procedures Unit Code: 500311108Document3 pagesUnit of Competency: Practice Occupational Health and Safety Procedures Unit Code: 500311108mvgeNo ratings yet
- Changing Our Understanding of HealthDocument4 pagesChanging Our Understanding of HealthYuliana DewiNo ratings yet
- First Aid For Snake BitesDocument15 pagesFirst Aid For Snake BitesMary Grace OgatisNo ratings yet
- Brazilian Journal of Physical TherapyDocument12 pagesBrazilian Journal of Physical TherapyKen ABNo ratings yet
- Self-Quarantine: Procedures For Under Covid-19Document1 pageSelf-Quarantine: Procedures For Under Covid-19trúc thuyên nguyễnNo ratings yet