You might also like
- IPM-Service Report FormDocument3 pagesIPM-Service Report FormAiko Mara Villanueva50% (2)
- Roadwork Projects Quality Control PlanDocument17 pagesRoadwork Projects Quality Control PlanSPHERICBLUE100% (2)
- Encyclopedia of Chemical Processing and Design. 69 - Supplement 1Document277 pagesEncyclopedia of Chemical Processing and Design. 69 - Supplement 1steamboatpirate80% (15)
- Chapter 3 ExercisesDocument3 pagesChapter 3 ExercisesKidGhost50% (2)
- NewbornDocument45 pagesNewbornkiran kumarNo ratings yet
- Nicu ReportDocument18 pagesNicu ReportKabita KarakNo ratings yet
- Tubal Patency TestDocument3 pagesTubal Patency TestLovely SarangiNo ratings yet
- Pessary InsertionDocument2 pagesPessary InsertionMutia LailaniNo ratings yet
- Induction of LaborDocument46 pagesInduction of Laborzamurd76No ratings yet
- Assignment On Obstetrics and Gynaecology DepartmentDocument14 pagesAssignment On Obstetrics and Gynaecology Departmentbhavnil_1796No ratings yet
- Baby Friendly Hospital Initiative (Bfhi)Document9 pagesBaby Friendly Hospital Initiative (Bfhi)Ankita BramheNo ratings yet
- Augmentation of Labour: Nabhan A, Boulvain MDocument8 pagesAugmentation of Labour: Nabhan A, Boulvain MMade SuryaNo ratings yet
- Integrated Child Development Services PresentationDocument33 pagesIntegrated Child Development Services PresentationNamitha Elizabeth Mani100% (1)
- PREMATURITYDocument40 pagesPREMATURITYBlykeBantuganNo ratings yet
- Maternal and Perinatal Outcome in Jaundice Complicating PregnancyDocument10 pagesMaternal and Perinatal Outcome in Jaundice Complicating PregnancymanognaaaaNo ratings yet
- DialysisDocument20 pagesDialysisSiwani rai100% (1)
- Radiant WarmersDocument5 pagesRadiant WarmersUday KumarNo ratings yet
- Psychiatric Disorders During PregnancyDocument28 pagesPsychiatric Disorders During PregnancyLamnunnem Haokip100% (1)
- Maternal and Child Health CareDocument12 pagesMaternal and Child Health CarePraachii SharmaNo ratings yet
- 10 Nurses Proper Professional EtiquetteDocument1 page10 Nurses Proper Professional EtiquetteReva stevanaNo ratings yet
- A Study To Evaluate The Effectiveness of Structured Teaching Program On Knowledge and Practice Regarding Kangaroo Mother Care Among Post Natal Mothers Having Low Birth Weight Babies 1Document9 pagesA Study To Evaluate The Effectiveness of Structured Teaching Program On Knowledge and Practice Regarding Kangaroo Mother Care Among Post Natal Mothers Having Low Birth Weight Babies 1Manisa ParidaNo ratings yet
- Janani Shishu Suraksha KaryakramDocument2 pagesJanani Shishu Suraksha KaryakramNeeraj Bhargav0% (1)
- Incubator Care 1Document4 pagesIncubator Care 1Mayank KumarNo ratings yet
- Newborn AssessmentDocument9 pagesNewborn Assessmentapi-237668254No ratings yet
- Prolonged LabourDocument3 pagesProlonged Labourannu panchalNo ratings yet
- Care of Child in IncubatorDocument12 pagesCare of Child in IncubatorSundaraBharathiNo ratings yet
- Adoption Laws in India - RidhiDocument5 pagesAdoption Laws in India - Ridhivarunendra pandeyNo ratings yet
- Ivf AssignmentDocument4 pagesIvf AssignmentNadiya RashidNo ratings yet
- Review of Literature On Temporary Family Planning MethodsDocument5 pagesReview of Literature On Temporary Family Planning MethodsafdtjozlbNo ratings yet
- Breast FeedingDocument3 pagesBreast FeedingArla Donissa-Donique Castillon AlviorNo ratings yet
- Preconception Care Presentation SlidesDocument15 pagesPreconception Care Presentation SlidesLucy AsconaNo ratings yet
- Female FoeticideDocument16 pagesFemale FoeticideSimran Singh MassaunNo ratings yet
- High-Risk NCM 102Document36 pagesHigh-Risk NCM 102EmmanuelL.TarucNo ratings yet
- Report - For MaamDocument7 pagesReport - For MaamSherchen Antonio-CortesNo ratings yet
- Kathryn E. Barnard: Athina Karla C. Chia, RNDocument8 pagesKathryn E. Barnard: Athina Karla C. Chia, RNMilagros FloritaNo ratings yet
- 1.1, 1.2, 1.3, 1.5 Paediatric Nursing Presentation - 1-1Document54 pages1.1, 1.2, 1.3, 1.5 Paediatric Nursing Presentation - 1-1Christina YounasNo ratings yet
- 2antenatal CareDocument10 pages2antenatal CareuouoNo ratings yet
- Pelvic Inflammatory DiseaseDocument15 pagesPelvic Inflammatory DiseaseJay PaulNo ratings yet
- Puerperal SepsisDocument4 pagesPuerperal SepsisSonali NayakNo ratings yet
- To Assess The Knowledge On Prevention and Control of Worm Infestations Among The Mothers' of Underfive Children at Erode, TamilnaduDocument3 pagesTo Assess The Knowledge On Prevention and Control of Worm Infestations Among The Mothers' of Underfive Children at Erode, TamilnaduInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pelvic Inflammatory DiseaseDocument9 pagesPelvic Inflammatory DiseaseanweshaNo ratings yet
- Pregnancy Induced HypertensionDocument52 pagesPregnancy Induced HypertensionJoy GloryNo ratings yet
- LegalaspectsDocument47 pagesLegalaspectssanthiyasandy100% (1)
- Joy Zachariah's Case Study.Document11 pagesJoy Zachariah's Case Study.Kuto Yvonne CheronoNo ratings yet
- Prenatal CareDocument64 pagesPrenatal CareAmy LalringhluaniNo ratings yet
- Hypertensive Disorders of Pregnancy: Mohammad Khalandar (116) Megha DDocument22 pagesHypertensive Disorders of Pregnancy: Mohammad Khalandar (116) Megha DMegha D100% (1)
- Intrauterine Growth Restriction IUGR: TH THDocument2 pagesIntrauterine Growth Restriction IUGR: TH THZahra AlaradiNo ratings yet
- Harika Priyanka. K Asst. Professor AconDocument30 pagesHarika Priyanka. K Asst. Professor AconArchana MoreyNo ratings yet
- Newborn Thermoregulation SLM 2013 06Document16 pagesNewborn Thermoregulation SLM 2013 06Fatimata SariNo ratings yet
- Post Mastectomy ExerciseDocument4 pagesPost Mastectomy ExerciseKusum RoyNo ratings yet
- Practice Teaching Demonstration: Intracath InsertionDocument13 pagesPractice Teaching Demonstration: Intracath InsertionMegha lakra100% (1)
- Teachers Role in Managing Non Projected ADocument23 pagesTeachers Role in Managing Non Projected Amanju meenaNo ratings yet
- Subinvolution of The UterusDocument5 pagesSubinvolution of The UterusJanica Rose Maloloy-onNo ratings yet
- First Referral UnitDocument24 pagesFirst Referral Unitjay5ar5jamorabon5torNo ratings yet
- Miconazole (Monistat) For 7 Flucanazole (Diflucan)Document8 pagesMiconazole (Monistat) For 7 Flucanazole (Diflucan)JimoiNo ratings yet
- PostnatalDocument36 pagesPostnatalAditya BarmanNo ratings yet
- SUCADENUMDocument9 pagesSUCADENUMmayliaNo ratings yet
- Management of Breast FeedingDocument17 pagesManagement of Breast FeedingUday KumarNo ratings yet
- An Exploratory Study To Assess The Knowledge Among Mothers of Under Five Children Regarding Thumb Sucking in Selected Village of MogaDocument58 pagesAn Exploratory Study To Assess The Knowledge Among Mothers of Under Five Children Regarding Thumb Sucking in Selected Village of MogaVarun JainNo ratings yet
- Physiologic Adaptation of The Newborn and Nursing AssessmentDocument108 pagesPhysiologic Adaptation of The Newborn and Nursing AssessmentRevathi DadamNo ratings yet
- ICDSDocument30 pagesICDSMadhu Ranjan100% (1)
- Kangaroo Mother CareDocument9 pagesKangaroo Mother CareSREEDEVI T SURESHNo ratings yet
- NICU OrganizationDocument5 pagesNICU Organizationgopscharan100% (1)
- NICUDocument15 pagesNICUSUSHMITHA.L sushmiNo ratings yet
- MPC5748GRMDocument4,039 pagesMPC5748GRMTaoufik BelkebirNo ratings yet
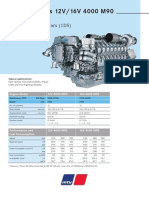
- Diesel Engines 12V/16V 4000 M90: For Vessels With Low Load Factors (1DS)Document2 pagesDiesel Engines 12V/16V 4000 M90: For Vessels With Low Load Factors (1DS)Alberto100% (1)
- Active Directory Offline Hash Dump and ForensicsDocument10 pagesActive Directory Offline Hash Dump and ForensicsHung NguyenNo ratings yet
- Relay Module - PLC-RSC-24DC/21 - 2966171: Key Commercial DataDocument15 pagesRelay Module - PLC-RSC-24DC/21 - 2966171: Key Commercial Datasatheez3251No ratings yet
- Circuit Theory Ch09Document30 pagesCircuit Theory Ch09최창하 ERICA 전자공학부No ratings yet
- Car Parking System Using IOT FinlDocument12 pagesCar Parking System Using IOT FinlCodingMasterNo ratings yet
- Price List: Reinforced ConcreteDocument16 pagesPrice List: Reinforced ConcreteLyjie BernabeNo ratings yet
- Philips Xh3 HP l1502 l1523 Compaq Fp5315Document65 pagesPhilips Xh3 HP l1502 l1523 Compaq Fp5315BAAAKNo ratings yet
- Vectornate Fogging Machine CatalogDocument32 pagesVectornate Fogging Machine CatalogMd.Tareque AbdullahNo ratings yet
- Chapter 4 AXial Loading MemberDocument20 pagesChapter 4 AXial Loading Memberk.ghanemNo ratings yet
- Foam Calculation Sample From ForumDocument2 pagesFoam Calculation Sample From Forumika524No ratings yet
- Wolf Sanoclav Sterilizer KL, TKL-MCS - User Manual-1Document10 pagesWolf Sanoclav Sterilizer KL, TKL-MCS - User Manual-1DirkNo ratings yet
- Iso 21940 1 2019Document12 pagesIso 21940 1 2019Inspección refamecaNo ratings yet
- One-Dimensional ProblemsDocument45 pagesOne-Dimensional Problemsajith kumarNo ratings yet
- Revised Courses Scheme: 91 Senate Approved Courses Scheme & Syllabus For B.E. Civil Engg. (2016)Document89 pagesRevised Courses Scheme: 91 Senate Approved Courses Scheme & Syllabus For B.E. Civil Engg. (2016)Rahul SehgalNo ratings yet
- Tutorial 7 Div1A2A2B3BDocument2 pagesTutorial 7 Div1A2A2B3BAnimesh SinghNo ratings yet
- DC 2.875 18 1.250id 2.375htpac SpiralDocument1 pageDC 2.875 18 1.250id 2.375htpac SpiralGarcia MarinNo ratings yet
- Project-Proposal-Thea ArroyoDocument5 pagesProject-Proposal-Thea ArroyoThea QuibuyenNo ratings yet
- Pka-Rp60Kal - TH Pka-Rp71Kal - TH PKA-RP100KAL - TH: Service ManualDocument32 pagesPka-Rp60Kal - TH Pka-Rp71Kal - TH PKA-RP100KAL - TH: Service ManualВладимир НаумычNo ratings yet
- Fluke 3031-3032 User ManualDocument36 pagesFluke 3031-3032 User ManualMeraj AlamNo ratings yet
- I ( (RC Theories - Ch. 1, 2, 3) ) I ( ( (Part A) ) ) - QZ.1&2 & HW.1&2 & Exam-1Document96 pagesI ( (RC Theories - Ch. 1, 2, 3) ) I ( ( (Part A) ) ) - QZ.1&2 & HW.1&2 & Exam-1Eng MuazNo ratings yet
- Hybrid Composite. An MMC Is Complementary To A Cermet. CompositionDocument5 pagesHybrid Composite. An MMC Is Complementary To A Cermet. Compositionvishnu_prasathNo ratings yet
- Shop Manual DL300-3 / DL350-3 Wheel Loader: Serial Number 10001 and UpDocument21 pagesShop Manual DL300-3 / DL350-3 Wheel Loader: Serial Number 10001 and UpСестрички Смайл50% (2)
- MultigradeTransmissionAndDriveTrainOilRequirementsTO 4MDocument69 pagesMultigradeTransmissionAndDriveTrainOilRequirementsTO 4MJosé JaegerNo ratings yet
- Usb FobDocument22 pagesUsb FobvcomuaNo ratings yet