You might also like
- Activity Sheet For Physical Education 2Document12 pagesActivity Sheet For Physical Education 2Elmer GornezNo ratings yet
- Back Hypertrophy Pull-Push-LegsDocument8 pagesBack Hypertrophy Pull-Push-LegsRohan PangotraaNo ratings yet
- 4-Week Total Body Program Part 1Document60 pages4-Week Total Body Program Part 1lehliemNo ratings yet
- Free Gym PlansDocument8 pagesFree Gym Plansmar s100% (1)
- ETK Erin Killeen TransformDocument16 pagesETK Erin Killeen Transformanabanana2No ratings yet
- 15minutes To FitDocument272 pages15minutes To FitLynsey100% (2)
- Pilates E-SsentialsDocument75 pagesPilates E-SsentialsPina Olson CampbellNo ratings yet
- Cycling Test ProtocolDocument7 pagesCycling Test ProtocolJonathan Bradley TepplerNo ratings yet
- Exercise Prescription ElementsDocument6 pagesExercise Prescription ElementsIrish Gamboa Duenas100% (1)
- KarlLifts Training Plan Copy (Template)Document20 pagesKarlLifts Training Plan Copy (Template)Luca A.No ratings yet
- Huge Harambe ProgramDocument17 pagesHuge Harambe Programblaha100% (1)
- Body Alchemy: The Shredded AcademyDocument6 pagesBody Alchemy: The Shredded AcademyMATHEWS MATHEWSNo ratings yet
- Classical Approach to Constrained and Unconstrained Molecular DynamicsFrom EverandClassical Approach to Constrained and Unconstrained Molecular DynamicsNo ratings yet
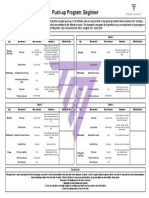
- Push Up Program BeginnerDocument1 pagePush Up Program BeginnerGavin ChhuorNo ratings yet
- 80/20 Endurance: The Complete System for High-Performance CoachingFrom Everand80/20 Endurance: The Complete System for High-Performance CoachingNo ratings yet
- Swimming Paper PDFDocument243 pagesSwimming Paper PDFRagini AdhikariNo ratings yet
- Prediction of Race Walking Performance Via LaDocument7 pagesPrediction of Race Walking Performance Via LaJuan AvilaNo ratings yet
- Scheer 2018Document6 pagesScheer 2018Einar Cumplido MartínezNo ratings yet
- IJSM - 29 - 453-459 - 2008 - Pace e RPEDocument7 pagesIJSM - 29 - 453-459 - 2008 - Pace e RPEWellington VicenteNo ratings yet
- RBCDH: Performance Prediction of Endurance Runners Through Laboratory and Track TestsDocument10 pagesRBCDH: Performance Prediction of Endurance Runners Through Laboratory and Track TestsBrayan Estiben Agudelo RodriguezNo ratings yet
- 10 1 1 552 171 PDFDocument8 pages10 1 1 552 171 PDFA'sHaikalNo ratings yet
- Rowing PDFDocument8 pagesRowing PDFkullNo ratings yet
- 573-Article Text-2914-1-10-20201228Document2 pages573-Article Text-2914-1-10-20201228FADHLAN ARISNo ratings yet
- Preprint Mazza OOxygen Uptakein Female RowersDocument10 pagesPreprint Mazza OOxygen Uptakein Female Rowersstrokeman75No ratings yet
- Effects of High Intensity Training by Heart Rate.34Document7 pagesEffects of High Intensity Training by Heart Rate.34Maxwell MartinsNo ratings yet
- JEP Journal of Exercise Physiology: OnlineDocument8 pagesJEP Journal of Exercise Physiology: OnlineMuthu GopalNo ratings yet
- A Maximal Rowing Ergometer Protocol To Predict MaxDocument9 pagesA Maximal Rowing Ergometer Protocol To Predict Maxstrokeman75No ratings yet
- Exercise Tests Cúrrente Situación and Furrier ProspectivasDocument10 pagesExercise Tests Cúrrente Situación and Furrier ProspectivasnataliecallegNo ratings yet
- Abs TrakDocument2 pagesAbs Trakrahmat khairulNo ratings yet
- New Equations Estimate College Students' Max Oxygen UptakeDocument6 pagesNew Equations Estimate College Students' Max Oxygen UptakeKıymet KayaNo ratings yet
- Effects of A Race Timer On The 3MT For Critical PowerDocument8 pagesEffects of A Race Timer On The 3MT For Critical PowerLéaNo ratings yet
- Ijerph 17 09250 v2Document11 pagesIjerph 17 09250 v2Brayan Estiben Agudelo RodriguezNo ratings yet
- 01 The Physiology of The World Record Holder - DR Andrew JonesDocument16 pages01 The Physiology of The World Record Holder - DR Andrew JonesbiratãNo ratings yet
- (Polish Journal of Sport and Tourism) The Estimation of The RAST Test Usefulness in Monitoring The Anaerobic Capacity of Sprinters in AthleticsDocument5 pages(Polish Journal of Sport and Tourism) The Estimation of The RAST Test Usefulness in Monitoring The Anaerobic Capacity of Sprinters in AthleticsAfizieNo ratings yet
- Jappl 1997 82 2 661Document6 pagesJappl 1997 82 2 661GilqlobroNo ratings yet
- Performance During A 20-km Cycling Time-Trial After Caffeine IngestionDocument7 pagesPerformance During A 20-km Cycling Time-Trial After Caffeine IngestionCristianLopezNo ratings yet
- Augmented Cooper Test Biomechanical ContributionsDocument16 pagesAugmented Cooper Test Biomechanical ContributionsFabiano LacerdaNo ratings yet
- Relationship between SSC tests and sprint performance in female athletesDocument6 pagesRelationship between SSC tests and sprint performance in female athleteslinoco1No ratings yet
- Eugenio 9933 PDF 56099 6 10 20201001 1Document6 pagesEugenio 9933 PDF 56099 6 10 20201001 1Yared TegegneNo ratings yet
- A Progressive Shuttle Run TestDocument5 pagesA Progressive Shuttle Run TestLing Lii LikNo ratings yet
- Clark 2010Document9 pagesClark 2010asepsumpenaNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleAnonymous 07vOE7U31LNo ratings yet
- Effects of Stage Duration in Incremental Running Tests On Physio 2003Document6 pagesEffects of Stage Duration in Incremental Running Tests On Physio 2003João VitorNo ratings yet
- Effects of A Plyometrics Intervention Program On Sprint PerformanceDocument7 pagesEffects of A Plyometrics Intervention Program On Sprint Performancenachox_99No ratings yet
- Training Periodization, Methods, Intensity Distribution, and Volume in Highly Trained and Elite Distance RunnersDocument14 pagesTraining Periodization, Methods, Intensity Distribution, and Volume in Highly Trained and Elite Distance RunnersJAIME FERNÁNDEZ FERNÁNDEZNo ratings yet
- Validation of GPS and Accelerometer Technology in SwimmingDocument5 pagesValidation of GPS and Accelerometer Technology in SwimmingAuguste LanconNo ratings yet
- Effects of plyometric training and drop jumps on 5-km running performanceDocument14 pagesEffects of plyometric training and drop jumps on 5-km running performancePriyanka ChoursiyaNo ratings yet
- 1 Grivas TSS 2020 273 117-123Document7 pages1 Grivas TSS 2020 273 117-123Yared TegegneNo ratings yet
- Comparison of Treadmill Based and Track Based Rockport 1 Mile Walk Test For Estimating Aerobic Capacity in Healthy Adults Ages 30-50 YearsDocument4 pagesComparison of Treadmill Based and Track Based Rockport 1 Mile Walk Test For Estimating Aerobic Capacity in Healthy Adults Ages 30-50 Yearsmanjula dangeNo ratings yet
- The Effects of High-Intensity Interval Training in Well-Trained RowersDocument12 pagesThe Effects of High-Intensity Interval Training in Well-Trained RowersDavid Ruiz GonzalezNo ratings yet
- 2d Endurance TrainDocument26 pages2d Endurance TrainJasunNo ratings yet
- Validity of The Running Anaerobic Sprint Test (Rast) For Assess Anaerobic Power and Predicting Performances: 2138Document9 pagesValidity of The Running Anaerobic Sprint Test (Rast) For Assess Anaerobic Power and Predicting Performances: 2138Nur CahyoNo ratings yet
- Quantifying The Training-Intensity Distribution in Middle-Distance Runners - The Influence of Different Methods of Training-Intensity QuantificationDocument6 pagesQuantifying The Training-Intensity Distribution in Middle-Distance Runners - The Influence of Different Methods of Training-Intensity QuantificationDouglas MarinNo ratings yet
- 13 2 2023 SubmaximalDocument13 pages13 2 2023 SubmaximalbiosoccerNo ratings yet
- The Acceleration Dependent Validity and Rel - 2014 - Journal of Science and MediDocument5 pagesThe Acceleration Dependent Validity and Rel - 2014 - Journal of Science and MedidrexalvesNo ratings yet
- A Five Year Physiological Case Study of An Olympic RunnerDocument5 pagesA Five Year Physiological Case Study of An Olympic RunnerAzarias Del Rosario CastilloNo ratings yet
- Materi 1 - WS Exercise Stress TestDocument25 pagesMateri 1 - WS Exercise Stress TestMaria ulfahNo ratings yet
- Positive Effects of Augmented Feedback To Reduce Time On Ground in Well-Trained RunnersDocument8 pagesPositive Effects of Augmented Feedback To Reduce Time On Ground in Well-Trained RunnersBenjapol BenjapalakornNo ratings yet
- The Effects of 8-Week Speed Training Program On The Acceleration Ability and Maximum Speed Running at 11 Years AthletesDocument8 pagesThe Effects of 8-Week Speed Training Program On The Acceleration Ability and Maximum Speed Running at 11 Years AthletesCesar Adolfo Ortega VivasNo ratings yet
- Multi-Stage 20-m Shuttle Run Fitness Test, Maximal Oxygen Uptake and Velocity at Maximal Oxygen UptakeDocument7 pagesMulti-Stage 20-m Shuttle Run Fitness Test, Maximal Oxygen Uptake and Velocity at Maximal Oxygen UptakeAlifa Diar UtamieNo ratings yet
- Test of The Classic Model For Predicting Endurance.20Document7 pagesTest of The Classic Model For Predicting Endurance.20Gust AvoNo ratings yet
- Effects of A Seven Day Period of High-Intensity Training On Performance and Physiology of Competitive CyclistsDocument1 pageEffects of A Seven Day Period of High-Intensity Training On Performance and Physiology of Competitive CyclistsCristianLopezNo ratings yet
- Training Intensity Distribuition Analysis by Race Pace Vs Physiological Approach in World-Class Middle - and Long-Distance RunnersDocument24 pagesTraining Intensity Distribuition Analysis by Race Pace Vs Physiological Approach in World-Class Middle - and Long-Distance Runnersgines.gonzalez.umhNo ratings yet
- A Simple Method For Computing Sprint Acceleration Kinetics FromDocument6 pagesA Simple Method For Computing Sprint Acceleration Kinetics FromapapirioNo ratings yet
- Effect of Carbohydrate Mouth Rinsing On Multiple Sprint PerformanceDocument8 pagesEffect of Carbohydrate Mouth Rinsing On Multiple Sprint PerformanceJordiGimenezNo ratings yet
- Art 1Document3 pagesArt 1GutoGonçalvesNo ratings yet
- 12074-Article Text-45143-1-10-20180524Document7 pages12074-Article Text-45143-1-10-20180524Giliard Lago GarciaNo ratings yet
- Aerobic Capacity, Body Mass Index and Fat Fold Measurements of Healthy Athletes in Dehradun - A Cross Sectional Study SRJI Vol 2 Issue 3 Year 2013Document6 pagesAerobic Capacity, Body Mass Index and Fat Fold Measurements of Healthy Athletes in Dehradun - A Cross Sectional Study SRJI Vol 2 Issue 3 Year 2013Dr. Krishna N. SharmaNo ratings yet
- Yo-Yo Intermittent Recovery Level 2Document4 pagesYo-Yo Intermittent Recovery Level 2DJNo ratings yet
- Average VO2Máx As A Function of Running Performances On Different DistancesDocument7 pagesAverage VO2Máx As A Function of Running Performances On Different DistancesCristianLopezNo ratings yet
- HM_Art_38656-10Document7 pagesHM_Art_38656-10陈韦杰No ratings yet
- Influencia Del Oxigeno en La KinematicaDocument25 pagesInfluencia Del Oxigeno en La KinematicaManuel GonzalezNo ratings yet
- Articulo Funcional ExposicionDocument12 pagesArticulo Funcional ExposicionBrayan Estiben Agudelo RodriguezNo ratings yet
- Reaction Time and Anticipatory Skill of Athletes in Open and Closed Skill-Dominated SportDocument8 pagesReaction Time and Anticipatory Skill of Athletes in Open and Closed Skill-Dominated SportLizette Camila Martinez AguillónNo ratings yet
- Swimming Canada Planning Long TermDocument40 pagesSwimming Canada Planning Long TermAnechitei Mihai-GabrielNo ratings yet
- Effects of Strength Training On The Physiological Determinants of Middle-And Long-Distance Running Performance: A Systematic ReviewDocument33 pagesEffects of Strength Training On The Physiological Determinants of Middle-And Long-Distance Running Performance: A Systematic ReviewAlexandre FerreiraNo ratings yet
- accedaCRIS Export PDFDocument2 pagesaccedaCRIS Export PDFBrayan Estiben Agudelo RodriguezNo ratings yet
- Effects of Strength Training On The Physiological Determinants of Middle-And Long-Distance Running Performance: A Systematic ReviewDocument33 pagesEffects of Strength Training On The Physiological Determinants of Middle-And Long-Distance Running Performance: A Systematic ReviewAlexandre FerreiraNo ratings yet
- Reaction Time and Anticipatory Skill of Athletes in Open and Closed Skill-Dominated SportDocument8 pagesReaction Time and Anticipatory Skill of Athletes in Open and Closed Skill-Dominated SportLizette Camila Martinez AguillónNo ratings yet
- One at A Time: LGBTQ Polyamory and Relational Citizenship in The 21st CenturyDocument17 pagesOne at A Time: LGBTQ Polyamory and Relational Citizenship in The 21st CenturyBrayan Estiben Agudelo RodriguezNo ratings yet
- 2019.cerezuelaetal - anovelshorttracktestMAS ShortDocument2 pages2019.cerezuelaetal - anovelshorttracktestMAS ShortBrayan Estiben Agudelo RodriguezNo ratings yet
- Ijerph 17 09250 v2Document11 pagesIjerph 17 09250 v2Brayan Estiben Agudelo RodriguezNo ratings yet
- 2019.cerezuelaetal - anovelshorttracktestMAS ShortDocument2 pages2019.cerezuelaetal - anovelshorttracktestMAS ShortBrayan Estiben Agudelo RodriguezNo ratings yet
- Predictive Performance Models in Long-Distance (2020)Document23 pagesPredictive Performance Models in Long-Distance (2020)BastianRiverosVasquezNo ratings yet
- Ijerph 17 09250 v2Document11 pagesIjerph 17 09250 v2Brayan Estiben Agudelo RodriguezNo ratings yet
- Effects of Strength Training On The Physiological Determinants of Middle-And Long-Distance Running Performance: A Systematic ReviewDocument33 pagesEffects of Strength Training On The Physiological Determinants of Middle-And Long-Distance Running Performance: A Systematic ReviewBrayan Estiben Agudelo RodriguezNo ratings yet
- Peerj 07 6787Document21 pagesPeerj 07 6787Brayan Estiben Agudelo RodriguezNo ratings yet
- David Laid DUP EditedDocument12 pagesDavid Laid DUP EditedJ4ChU -M-No ratings yet
- Rutina Calistenia Mejorada 1.0 HipertrofiaDocument6 pagesRutina Calistenia Mejorada 1.0 HipertrofiakevinNo ratings yet
- Physical Fitness Workout PlanDocument2 pagesPhysical Fitness Workout PlanJohn Vincent SemillanoNo ratings yet
- HOPE 3 Module 2Document28 pagesHOPE 3 Module 2Deey Lanne Casuga RufintaNo ratings yet
- 9 Squat Accessories To Improve Strength Technique 1Document13 pages9 Squat Accessories To Improve Strength Technique 1Alejandro Herrnsdorf-SakellaridisNo ratings yet
- The New One-Day Arm CureDocument16 pagesThe New One-Day Arm CureJoseph GlaserNo ratings yet
- Benefits of Aerobics, Zumba, Pilates, and Tae BoDocument3 pagesBenefits of Aerobics, Zumba, Pilates, and Tae BoTRIXIEJOY INIONNo ratings yet
- q1 Grade 8 Synchronous Revised Fitness-Test-Score-CardDocument1 pageq1 Grade 8 Synchronous Revised Fitness-Test-Score-CardAlbert Ian CasugaNo ratings yet
- David, Joshua B. - PE - Module 6 - ActivitiesDocument5 pagesDavid, Joshua B. - PE - Module 6 - ActivitiesHanah Grace GomezNo ratings yet
- Importance of Horizontally Loaded Movements To Sports PerformanceDocument7 pagesImportance of Horizontally Loaded Movements To Sports Performancederamos10No ratings yet
- TSA Beginner ApproachDocument122 pagesTSA Beginner ApproachmacarifficNo ratings yet
- Boxing Science HIIT Beginner Programme OUTDOORSDocument41 pagesBoxing Science HIIT Beginner Programme OUTDOORSalexunder94No ratings yet
- LM+Challenge Game Changer V4 9nov21Document38 pagesLM+Challenge Game Changer V4 9nov21Tang SeNo ratings yet
- Periodization Training for Sports (Tudor Bompa, Carlo Buzzichelli) (z-lib.org)_1Document36 pagesPeriodization Training for Sports (Tudor Bompa, Carlo Buzzichelli) (z-lib.org)_1totofrudiNo ratings yet
- Carl Assessment MatrixDocument5 pagesCarl Assessment Matrixapi-569132011No ratings yet
- For This CompositionDocument1 pageFor This Compositionmagyi skaNo ratings yet
- Module One Wellness PlanDocument9 pagesModule One Wellness PlanArson SkittlesNo ratings yet
- CORE151 MODULE06 TacataniDocument8 pagesCORE151 MODULE06 TacataniJho CamarinesNo ratings yet