You might also like
- 974-0753 Onan RDJC RDJF Diesel Engine Service Manual (09-1984)Document64 pages974-0753 Onan RDJC RDJF Diesel Engine Service Manual (09-1984)Leo BurnsNo ratings yet
- Burnout Syndrome in Critical Care Nursing StaffDocument7 pagesBurnout Syndrome in Critical Care Nursing Staffcallyope4No ratings yet
- The Word Became Flesh An Exploratory Essay On Jesu 003Document62 pagesThe Word Became Flesh An Exploratory Essay On Jesu 003Alexios VrionisNo ratings yet
- Meat PieDocument13 pagesMeat Piecrispitty100% (1)
- Revisi AHoJ Artikel PRAMITA DEWI - Id.enDocument5 pagesRevisi AHoJ Artikel PRAMITA DEWI - Id.enpramitadewi729No ratings yet
- 1471 244X 14 21Document7 pages1471 244X 14 21RiaNo ratings yet
- Revisi AHoJ Artikel PRAMITA DEWI - Id.enDocument5 pagesRevisi AHoJ Artikel PRAMITA DEWI - Id.enpramitadewi729No ratings yet
- 1941Document7 pages1941Zia CobosNo ratings yet
- A Study of Factors Influencing Psychological Stress Among Health Care Workers Providing Palliative and Hospice Care in Nursing DepartmentDocument8 pagesA Study of Factors Influencing Psychological Stress Among Health Care Workers Providing Palliative and Hospice Care in Nursing Departmentijsab.comNo ratings yet
- Pengaruh Kecemasan Terhadap PembedahanDocument6 pagesPengaruh Kecemasan Terhadap PembedahanRahmi Mutia UlfaNo ratings yet
- CC 12736Document8 pagesCC 12736Neneng HumairohNo ratings yet
- KAP Post Op Pain EthiopiaDocument6 pagesKAP Post Op Pain EthiopiaJehan AliodenNo ratings yet
- Nurses Knowledge Toward Cast Complications in Orthopedic Ward at Al-Najaf AL-Ashraf HospitalsDocument7 pagesNurses Knowledge Toward Cast Complications in Orthopedic Ward at Al-Najaf AL-Ashraf HospitalsZilbran BerontaxNo ratings yet
- 14186-Article Text-26331-5-10-20190611Document9 pages14186-Article Text-26331-5-10-20190611Al FatihNo ratings yet
- NoviDocument6 pagesNoviDAMIANNo ratings yet
- Medi 100 E25963Document4 pagesMedi 100 E25963LUIS AYALANo ratings yet
- A Community Based Program For PDFDocument9 pagesA Community Based Program For PDFana irianiNo ratings yet
- Mullaney 2015Document6 pagesMullaney 2015Angel Paz-JesusNo ratings yet
- Y G, N G, H G, J S 4, L S, X L 6, Y J: Anxia Uan A Uo Uining Ao Ian Un Ili Un Iaoping Iu An IangDocument5 pagesY G, N G, H G, J S 4, L S, X L 6, Y J: Anxia Uan A Uo Uining Ao Ian Un Ili Un Iaoping Iu An IangDeo RizkyandriNo ratings yet
- Abraham Et Al-2018-Emergency Medicine AustralasiaDocument7 pagesAbraham Et Al-2018-Emergency Medicine AustralasiaAl FatihNo ratings yet
- International Emergency Nursing: SciencedirectDocument7 pagesInternational Emergency Nursing: SciencedirectKavin Zank JuniorNo ratings yet
- Prevalence of Musculoskeletal Disorders For NursesDocument39 pagesPrevalence of Musculoskeletal Disorders For NursesMiguel RuizNo ratings yet
- JMedLife 09 363Document6 pagesJMedLife 09 363Al FatihNo ratings yet
- Amira PresuurevulcerDocument59 pagesAmira PresuurevulcerrantiNo ratings yet
- Musculoskeletal Disorder Risk Factors Among Nursing Professionals in Low Resource Settings: A Cross-Sectional Study in UgandaDocument8 pagesMusculoskeletal Disorder Risk Factors Among Nursing Professionals in Low Resource Settings: A Cross-Sectional Study in UgandaMABELNo ratings yet
- BurnoutDocument23 pagesBurnoutAni NurcahyaniNo ratings yet
- Effectofcarereducationon Functionalabilitiesofpatients WithstrokeDocument7 pagesEffectofcarereducationon Functionalabilitiesofpatients WithstrokeDan Gerald Alcido SalungaNo ratings yet
- Resilience and Mental Health NursingDocument15 pagesResilience and Mental Health NursingDWNo ratings yet
- Job Satisfaction in NursingDocument7 pagesJob Satisfaction in NursingBanis Rihadatul AfifahNo ratings yet
- Work Stress and Gender-Dependent Coping Strategies in Anesthesiologists at A University HospitalDocument6 pagesWork Stress and Gender-Dependent Coping Strategies in Anesthesiologists at A University HospitalwidianoviantiiNo ratings yet
- Stroke Scales and Trajectory of Recovery A Major Concern For Patients and Nurses AlikeDocument7 pagesStroke Scales and Trajectory of Recovery A Major Concern For Patients and Nurses AlikeAnonymous XO9RqHhOgiNo ratings yet
- Adriaen S Sens 2015Document13 pagesAdriaen S Sens 2015PeepsNo ratings yet
- End of LifeDocument3 pagesEnd of LifeSiti Fatimahtusz07No ratings yet
- Measuring Anxiety in Surgical Patients Using A Visual Analogue ScaleDocument6 pagesMeasuring Anxiety in Surgical Patients Using A Visual Analogue ScaleRonnel Astronomo ArleguiNo ratings yet
- (2004) Psychosocial Effect of SARS On Hospital StaffDocument6 pages(2004) Psychosocial Effect of SARS On Hospital StaffDiyah CandraNo ratings yet
- 002 10080bam0809 7 15Document9 pages002 10080bam0809 7 15chaterinaNo ratings yet
- Literature Review of Post-Traumatic Stress Disorder in The Critical Care PDFDocument14 pagesLiterature Review of Post-Traumatic Stress Disorder in The Critical Care PDFOriza Zara SativaNo ratings yet
- JurnalDocument8 pagesJurnalAulia ElmaNo ratings yet
- Hubungan Antara Operasi Katarak Dengan Tingkat Kecemasan Pasien Katarak SenilisDocument11 pagesHubungan Antara Operasi Katarak Dengan Tingkat Kecemasan Pasien Katarak Senilistujuh kurcaciNo ratings yet
- Conflicus Azoulay 2009Document8 pagesConflicus Azoulay 2009RodrigoSachiFreitasNo ratings yet
- Published PDF 2390 6 AssessingtheLevelofStressandAnxietyinFamilyMembersofPatientsHos PitalizedintheSpecialCareUnitsDocument6 pagesPublished PDF 2390 6 AssessingtheLevelofStressandAnxietyinFamilyMembersofPatientsHos PitalizedintheSpecialCareUnitsYiyiz HertikaNo ratings yet
- Hair-Normalized Cortisol Waking Response As A Novel Biomarker of HPA Axis Activity Following Acute TraumaDocument9 pagesHair-Normalized Cortisol Waking Response As A Novel Biomarker of HPA Axis Activity Following Acute TraumawgNo ratings yet
- BURNOUTDocument17 pagesBURNOUTSahian Montserrat Angeles HortaNo ratings yet
- EffectivenessDocument8 pagesEffectivenessIntan DwiNo ratings yet
- Functioning of Stroke Survivors - A Validation of The ICF Core Set For Stroke in SwedenDocument9 pagesFunctioning of Stroke Survivors - A Validation of The ICF Core Set For Stroke in SwedenMuhammadMusa47No ratings yet
- Annals of Medicine and Surgery: Bareza Rezaei, Elahe Mousavi, Bahram Heshmati, Shaphagh AsadiDocument8 pagesAnnals of Medicine and Surgery: Bareza Rezaei, Elahe Mousavi, Bahram Heshmati, Shaphagh AsadiGeysel SuarezNo ratings yet
- Family Needs of Critically Ill Patients Admitted To The Intensive Care Unit, Comparison of Nurses and Family PerceptionDocument14 pagesFamily Needs of Critically Ill Patients Admitted To The Intensive Care Unit, Comparison of Nurses and Family PerceptionRiaNo ratings yet
- 2019 Damico PROs and PROMs in MSDocument6 pages2019 Damico PROs and PROMs in MSMaría Pía BalmacedaNo ratings yet
- Jurnal 3Document7 pagesJurnal 3kampret berbagiNo ratings yet
- Journal Pone 0154372 PDFDocument15 pagesJournal Pone 0154372 PDFrutnomleniNo ratings yet
- DOL Intolerancia DolorDocument8 pagesDOL Intolerancia DolorJorge Lucas JimenezNo ratings yet
- Hubungan Tingkat Kecemasan Dengan Kualitas Tidur Pasien Pre Operasi Di Rumah Sakit Umum Sundari MedanDocument9 pagesHubungan Tingkat Kecemasan Dengan Kualitas Tidur Pasien Pre Operasi Di Rumah Sakit Umum Sundari MedanElisabet Enga taraladuNo ratings yet
- Prevalence and Risk Factors of Depression, Anxiety, and Stress in A Cohort of Australian NursesDocument10 pagesPrevalence and Risk Factors of Depression, Anxiety, and Stress in A Cohort of Australian NursesYudha SugandaNo ratings yet
- Journal Trakeostomi 6Document16 pagesJournal Trakeostomi 6Fatimah ZahraNo ratings yet
- 1 s2.0 S1356689X01904266 MainDocument8 pages1 s2.0 S1356689X01904266 MainaramNo ratings yet
- The Lived Experience and Meaning of Stress in Acute Mental Health NursesDocument7 pagesThe Lived Experience and Meaning of Stress in Acute Mental Health NursesZANDRA GOROSPENo ratings yet
- Prin 17Document5 pagesPrin 17JULIANINo ratings yet
- Emergency Department Triage Scales and Their Components: A Systematic Review of The Scientific EvidenceDocument13 pagesEmergency Department Triage Scales and Their Components: A Systematic Review of The Scientific Evidencearofah hNo ratings yet
- Document PDFDocument13 pagesDocument PDFMuizhima MuizNo ratings yet
- Low Back Pain and Quality of Life in Staff of Mansoura University Main HospitalDocument6 pagesLow Back Pain and Quality of Life in Staff of Mansoura University Main HospitalAbdullah ElgeddawyNo ratings yet
- 10 1002@msc 1498Document13 pages10 1002@msc 1498Ricardo PietrobonNo ratings yet
- Burnout in Hospital Nurses: A Comparison of Internal, Surgery, Psychiatry and Burns WardsDocument6 pagesBurnout in Hospital Nurses: A Comparison of Internal, Surgery, Psychiatry and Burns WardsArthuro Dax DacurroNo ratings yet
- Principles of Adult Surgical Critical CareFrom EverandPrinciples of Adult Surgical Critical CareNiels D. MartinNo ratings yet
- Bash - Ls - FundamentalsDocument5 pagesBash - Ls - FundamentalsPradip ShahiNo ratings yet
- Smartvista On Nonstop: Latest Developments and EnhancementsDocument26 pagesSmartvista On Nonstop: Latest Developments and EnhancementsPradip ShahiNo ratings yet
- Quick-Installation NMSDocument21 pagesQuick-Installation NMSPradip ShahiNo ratings yet
- Gokarna Forest Resort: Salary SlipDocument7 pagesGokarna Forest Resort: Salary SlipPradip ShahiNo ratings yet
- Self-Perceived Burden in Palliative CareDocument5 pagesSelf-Perceived Burden in Palliative CarePradip ShahiNo ratings yet
- Quarantine - Issolation Leave FormDocument1 pageQuarantine - Issolation Leave FormPradip ShahiNo ratings yet
- Physio Book - Knee - V1Document27 pagesPhysio Book - Knee - V1Pradip ShahiNo ratings yet
- Grade 7-Advanced Science Environmental ScienceDocument8 pagesGrade 7-Advanced Science Environmental ScienceChrisel Luat LopezNo ratings yet
- Montague Street Cable Car, Wall Street FerryDocument23 pagesMontague Street Cable Car, Wall Street FerryBob DiamondNo ratings yet
- Toxicological Stability of Drugs: de Jesus, Adia Cavrinni G. Manalo, Alyssa ADocument42 pagesToxicological Stability of Drugs: de Jesus, Adia Cavrinni G. Manalo, Alyssa AAlyssa ManaloNo ratings yet
- Benguet Folktales Bases For Tracing Family BloodlineDocument17 pagesBenguet Folktales Bases For Tracing Family BloodlineJohn Rey PelilaNo ratings yet
- Ecs C42iix Rev C Vit m2400 1Document36 pagesEcs C42iix Rev C Vit m2400 1Victor Pic100% (1)
- Assignment 33 PDFDocument9 pagesAssignment 33 PDFsayan mukherjeeNo ratings yet
- S800 SCL SR - 2CCC413009B0201 PDFDocument16 pagesS800 SCL SR - 2CCC413009B0201 PDFBalan PalaniappanNo ratings yet
- Investigation Gr. 8Document6 pagesInvestigation Gr. 8Marthie van zylNo ratings yet
- SEC - Connection Guidelines - v3 - CleanDocument54 pagesSEC - Connection Guidelines - v3 - CleanFurqan HamidNo ratings yet
- PDS Syncade RADocument6 pagesPDS Syncade RAKeith userNo ratings yet
- Training Schedule April 2021 To March 22 - 0Document18 pagesTraining Schedule April 2021 To March 22 - 0sanrexiNo ratings yet
- 22.anaerobes (Part II)Document91 pages22.anaerobes (Part II)sigrid jaramilloNo ratings yet
- Datasheet - 74LS283 - Somador Binário Completo de 4 BitsDocument7 pagesDatasheet - 74LS283 - Somador Binário Completo de 4 BitsLucas CarvalhoNo ratings yet
- ActuatorsDocument24 pagesActuatorsharishcsharmaNo ratings yet
- 01-System Devices Configuration - Rev GDocument36 pages01-System Devices Configuration - Rev GPABITRA PATRANo ratings yet
- A Novel Wastewater Derived BiodieselDocument13 pagesA Novel Wastewater Derived BiodieselYuri ClaroNo ratings yet
- Proline Table-Top Machines Z005 Up To Z100: Product InformationDocument2 pagesProline Table-Top Machines Z005 Up To Z100: Product InformationErika Mae EnticoNo ratings yet
- Livro Vertex MACIOCIADocument62 pagesLivro Vertex MACIOCIAxandinhag100% (5)
- TrerwtsdsDocument167 pagesTrerwtsdsvinicius gomes duarteNo ratings yet
- Ps 0412 0612obh WDocument1 pagePs 0412 0612obh WHunterNo ratings yet
- Temba KauDocument50 pagesTemba KaufauzanNo ratings yet
- Fra Assignment 1Document11 pagesFra Assignment 1Ruchi SambhariaNo ratings yet
- Hydrogen Codes and Standards Workshop: Naser ChowdhuryDocument24 pagesHydrogen Codes and Standards Workshop: Naser ChowdhuryDiana DhominicNo ratings yet
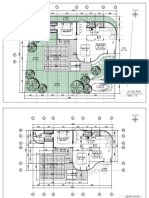
- 2023.01.25 Plan Pecatu Villa - FinishDocument3 pages2023.01.25 Plan Pecatu Villa - FinishTika AgungNo ratings yet
- Ground Power Unit: GA ModelDocument17 pagesGround Power Unit: GA ModelAngelica Nava0% (1)
- Blood Physiology 2022Document116 pagesBlood Physiology 2022Gurmessa FekaduNo ratings yet
- Catchment CharacterisationDocument48 pagesCatchment CharacterisationSherlock BaileyNo ratings yet