You might also like
- Introduction to Clinical Reproductive EndocrinologyFrom EverandIntroduction to Clinical Reproductive EndocrinologyRating: 1 out of 5 stars1/5 (1)
- Gynecology: 3.09 - AmenorrheaDocument13 pagesGynecology: 3.09 - AmenorrheaAnna Mae MarantanNo ratings yet
- AMENORRHEA: AN APPROACH FOR DIAGNOSISDocument41 pagesAMENORRHEA: AN APPROACH FOR DIAGNOSISarfahregarNo ratings yet
- Abnormal Uterine BleedingDocument36 pagesAbnormal Uterine BleedingPranshu Prajyot 67100% (1)
- AmenorrheaDocument23 pagesAmenorrheaKarmmanya Razahani PurnamaNo ratings yet
- Amenorrhea: Preceptor Dr. Ni Made Desy S., MM. SP - OG Editor Jasmine Nazila 1010221067Document18 pagesAmenorrhea: Preceptor Dr. Ni Made Desy S., MM. SP - OG Editor Jasmine Nazila 1010221067nugrapitaNo ratings yet
- Secondary Amenorrhea: DR Hanaa AlaniDocument44 pagesSecondary Amenorrhea: DR Hanaa AlaniAakashNo ratings yet
- Dr. Sharda Jain: Director: Secretary GeneralDocument91 pagesDr. Sharda Jain: Director: Secretary GeneraljijaniNo ratings yet
- Uterus TransplantationDocument28 pagesUterus TransplantationJayaprakash SivamaniNo ratings yet
- Dr. Shehla Jamal Assistant Professor: OBG S M S & RDocument69 pagesDr. Shehla Jamal Assistant Professor: OBG S M S & RAppy LoveNo ratings yet
- Secondary Amenorrhea by Ghulam MurtazaDocument14 pagesSecondary Amenorrhea by Ghulam MurtazaDr. Ghulam Murtaza Palh100% (1)
- Investigating Primary Amenorrhea CaseDocument23 pagesInvestigating Primary Amenorrhea CaseMohammed AbdulNo ratings yet
- Drugs - OBGDocument85 pagesDrugs - OBGKENEDYNo ratings yet
- Pelvic Organ ProlapseDocument68 pagesPelvic Organ ProlapseAlyanna CrisologoNo ratings yet
- VBAC Guide: Risks, Benefits & ManagementDocument12 pagesVBAC Guide: Risks, Benefits & Managementnyangara50% (2)
- AmenorrheaDocument41 pagesAmenorrheadoraNo ratings yet
- Instrumental Vaginal Delivery: Professor Roshan Ara QaziDocument27 pagesInstrumental Vaginal Delivery: Professor Roshan Ara Qazikaram008No ratings yet
- Antenatal Care During The First, SecondDocument85 pagesAntenatal Care During The First, SecondhemihemaNo ratings yet
- Abnormal Uterin ActionDocument65 pagesAbnormal Uterin Actionshweta raiNo ratings yet
- AUBDocument45 pagesAUBJBNo ratings yet
- Multiple PregnancyDocument71 pagesMultiple PregnancyAndre PutraNo ratings yet
- Multiple PregnancyDocument26 pagesMultiple PregnancyOmar mohamedNo ratings yet
- Obstetrics & GynaecologyDocument52 pagesObstetrics & GynaecologyBhattarai ShrinkhalaNo ratings yet
- Placenta PreviaDocument2 pagesPlacenta PreviaAnonymous 0C4OZmRNo ratings yet
- ACOG Practice Bulletin ObesityDocument2 pagesACOG Practice Bulletin Obesitynoella deckbarNo ratings yet
- Seminar 5 - Thyroid Disease in PregnancyDocument25 pagesSeminar 5 - Thyroid Disease in PregnancyHakimah K. SuhaimiNo ratings yet
- Obg Extra EdgeDocument201 pagesObg Extra EdgeabhishekbmcNo ratings yet
- Gynaecology Revision PDFDocument13 pagesGynaecology Revision PDFAadhi AadhiNo ratings yet
- Feto Pelvic DisproportionDocument10 pagesFeto Pelvic DisproportionIsrael WoseneNo ratings yet
- Fibroid in Pregnancy: Characteristics, Complications, and ManagementDocument11 pagesFibroid in Pregnancy: Characteristics, Complications, and ManagementAnonymous UHnQSkxLBDNo ratings yet
- Benign Disease of The UterusDocument27 pagesBenign Disease of The UterusnyangaraNo ratings yet
- Primary and Secondary AmenorrhoeaDocument72 pagesPrimary and Secondary Amenorrhoead clarkeNo ratings yet
- Menstrual DisordersDocument29 pagesMenstrual DisorderstuhinsinghNo ratings yet
- Post Term PregnancyDocument14 pagesPost Term PregnancySanthosh.S.UNo ratings yet
- Caesarean SectionDocument73 pagesCaesarean SectionBhattarai Shrinkhala100% (2)
- Fetal head position during descentDocument29 pagesFetal head position during descentعمر احمد شاكرNo ratings yet
- Hypoxia Classification Table - Physiological-CTGDocument1 pageHypoxia Classification Table - Physiological-CTGKhánh Nguyễn NgọcNo ratings yet
- Cervical Cancer Diagnosis and ManagementDocument128 pagesCervical Cancer Diagnosis and Managementnicewan0% (1)
- Understanding Uterine FibroidsDocument15 pagesUnderstanding Uterine FibroidsAnuradha RoopchandNo ratings yet
- Gynecology Topics: Uterine Prolapse, Amenorrhea, Dysfunctional Bleeding, PCOS, Infertility, Menopause (39Document101 pagesGynecology Topics: Uterine Prolapse, Amenorrhea, Dysfunctional Bleeding, PCOS, Infertility, Menopause (39jojolilimomo100% (1)
- Twin PregnancyDocument73 pagesTwin Pregnancykrishna mandalNo ratings yet
- Gynaecological AssessmentDocument110 pagesGynaecological AssessmentKripa SusanNo ratings yet
- COMPLETE Medical Disease in PregnancyDocument210 pagesCOMPLETE Medical Disease in PregnancyCHANDREN ARUMUGAMNo ratings yet
- Antepartum HemorrhageDocument105 pagesAntepartum HemorrhageBablablo LolaleNo ratings yet
- Unstable LieDocument7 pagesUnstable Lieapi-370504667% (3)
- Gyne History Taking PDFDocument6 pagesGyne History Taking PDFGokul AdarshNo ratings yet
- Development of Uterus and Congenital Anomalies: Done By: Jabir AL Araimi ID# 0333145Document21 pagesDevelopment of Uterus and Congenital Anomalies: Done By: Jabir AL Araimi ID# 0333145jabirNo ratings yet
- MENSTRUAL DISORDERS: CAUSES, DIAGNOSIS AND MANAGEMENTDocument36 pagesMENSTRUAL DISORDERS: CAUSES, DIAGNOSIS AND MANAGEMENTAkinbani MoyosoreNo ratings yet
- Abnormal Uterine ActionDocument36 pagesAbnormal Uterine ActionMed PoxNo ratings yet
- Transverse LieDocument32 pagesTransverse LieBharat ThapaNo ratings yet
- M.M. College of Nursing: Assignment ON Mild, Moderate and Severe Pre-EclampsiaDocument4 pagesM.M. College of Nursing: Assignment ON Mild, Moderate and Severe Pre-EclampsiaNadiya RashidNo ratings yet
- Operative Vaginal Delivery PDFDocument56 pagesOperative Vaginal Delivery PDFFarehan Md IsaNo ratings yet
- Physiological Changes of PregnancyDocument40 pagesPhysiological Changes of PregnancyAita AladianseNo ratings yet
- Malposition - Breech PresentationDocument133 pagesMalposition - Breech PresentationRadhakrishnan GovindanNo ratings yet
- Page 1 of 5: Guidelines/green-Top-Guidelines/gtg - 67 - Endometrial - Hyperplasia PDFDocument5 pagesPage 1 of 5: Guidelines/green-Top-Guidelines/gtg - 67 - Endometrial - Hyperplasia PDFfitrah fajrianiNo ratings yet
- Managing Multiple PregnanciesDocument33 pagesManaging Multiple PregnanciesAndi Farid ANo ratings yet
- Uterinefibroids 130120064643 Phpapp02Document73 pagesUterinefibroids 130120064643 Phpapp02Tharun KumarNo ratings yet
- Vasa PraeviaDocument3 pagesVasa PraeviaAngelica CabututanNo ratings yet
- Genetics For MrcogDocument4 pagesGenetics For MrcogsriniNo ratings yet
- First 5 Secrets PDFDocument19 pagesFirst 5 Secrets PDFRajath KS100% (1)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Social and Community Psychiatry (Dr. Hernandez)Document6 pagesSocial and Community Psychiatry (Dr. Hernandez)carmsNo ratings yet
- Hemostasis: PGI TIONLOC, Catrina PGI TOMWONG, Francis GaryDocument22 pagesHemostasis: PGI TIONLOC, Catrina PGI TOMWONG, Francis GarycarmsNo ratings yet
- Differential Diagnosis of Pleural Effusions: Review ArticleDocument0 pagesDifferential Diagnosis of Pleural Effusions: Review ArticleRona SetiawatiNo ratings yet
- 134 2012 Article 2542Document9 pages134 2012 Article 2542carmsNo ratings yet
- Updated Clinical Practice Guidelines for the Management of Dyslipidemia in the PhilippinesDocument100 pagesUpdated Clinical Practice Guidelines for the Management of Dyslipidemia in the PhilippinesBlue PielagoNo ratings yet
- Oral Antidiabetic DrugsDocument46 pagesOral Antidiabetic Drugscarms100% (1)
- First 5 Secrets PDFDocument19 pagesFirst 5 Secrets PDFRajath KS100% (1)
- ATA Tiroides PDFDocument133 pagesATA Tiroides PDFGloria Pg MontzeNo ratings yet
- 00 Management of Difficult To Treat AD 2013Document10 pages00 Management of Difficult To Treat AD 2013Brigita De VegaNo ratings yet
- Japanese Guidelines For Atopic Dermatitis 2020Document14 pagesJapanese Guidelines For Atopic Dermatitis 2020vieeveeNo ratings yet
- 00 Management of Difficult To Treat AD 2013Document10 pages00 Management of Difficult To Treat AD 2013Brigita De VegaNo ratings yet
- Isotretinoin Treatment For Acne and Risk of Depression: A Systematic Review and Meta-AnalysisDocument18 pagesIsotretinoin Treatment For Acne and Risk of Depression: A Systematic Review and Meta-Analysisyohanes22No ratings yet
- Isotretinoin Treatment For Acne and Risk of Depression: A Systematic Review and Meta-AnalysisDocument18 pagesIsotretinoin Treatment For Acne and Risk of Depression: A Systematic Review and Meta-Analysisyohanes22No ratings yet
- TOPNOTCH MEDICAL BOARD PREP - COMMON OB-GYN EMERGENCIESDocument8 pagesTOPNOTCH MEDICAL BOARD PREP - COMMON OB-GYN EMERGENCIEScarmsNo ratings yet
- Technical Analysis GuideDocument175 pagesTechnical Analysis GuidecarmsNo ratings yet
- Philippine COVID-19 Living RecommendationsDocument19 pagesPhilippine COVID-19 Living RecommendationscarmsNo ratings yet
- Joseph Brian L. Costiniano, MD, DPCPDocument70 pagesJoseph Brian L. Costiniano, MD, DPCPcarmsNo ratings yet
- MCQs Distribution in OBG ExamDocument3 pagesMCQs Distribution in OBG ExamNatosha MendozaNo ratings yet
- I. Learning Objective:: /endocrine-System-Lesson-Plan-Final-Na-FinalDocument10 pagesI. Learning Objective:: /endocrine-System-Lesson-Plan-Final-Na-FinalGabilan Rose JeanNo ratings yet
- GENDSO Midterms NOTES.Document6 pagesGENDSO Midterms NOTES.Justin AprueboNo ratings yet
- Gynecology - Secondary AmenorrheaDocument2 pagesGynecology - Secondary AmenorrheaAnsley MadalaNo ratings yet
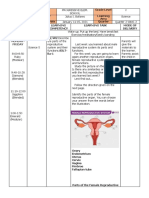
- Anatomy Physiology of Female Reproductive SystemDocument96 pagesAnatomy Physiology of Female Reproductive SystemRabin BasnetNo ratings yet
- Abnormal Uterine Bleeding Causes and TreatmentDocument29 pagesAbnormal Uterine Bleeding Causes and TreatmentJed Mostajo100% (2)
- CBSE NCERT Solutions For Class 12 Science Chapter 4: Back of Chapter QuestionsDocument5 pagesCBSE NCERT Solutions For Class 12 Science Chapter 4: Back of Chapter QuestionsSatvik MishraNo ratings yet
- Normal PuerperiumDocument12 pagesNormal PuerperiumAhmed TarigNo ratings yet
- Menstrual Cycle Feedback MechanismsDocument18 pagesMenstrual Cycle Feedback MechanismsAnonymous o3ZKP646E7100% (1)
- Week 2Document3 pagesWeek 2Ruiz Von LaguneroNo ratings yet
- Sexual Health and Fertility ClassDocument14 pagesSexual Health and Fertility ClassJaymih Santos AbasoloNo ratings yet
- XII Breast and Nipple ConditionsDocument23 pagesXII Breast and Nipple ConditionsteabagmanNo ratings yet
- BRS Peds NotesDocument57 pagesBRS Peds NotesRkkNo ratings yet
- Goboy, Louise Germaine U. BSN 210 Self-Assessment QuestionsDocument2 pagesGoboy, Louise Germaine U. BSN 210 Self-Assessment QuestionsLouise GermaineNo ratings yet
- OBSTETRICSMock BoardsDocument17 pagesOBSTETRICSMock BoardsDominque RabastoNo ratings yet
- Ob / Gyn Nursing: by Group 1 Elfa Susanti Nurafianti OktamegaDocument11 pagesOb / Gyn Nursing: by Group 1 Elfa Susanti Nurafianti OktamegaRolli SptNo ratings yet
- Growth and Development in ChildrenDocument118 pagesGrowth and Development in Childrenkrishnasree100% (6)
- Module 9 Adolescence Physical Cognitive and Socioemotional DevelopmentDocument23 pagesModule 9 Adolescence Physical Cognitive and Socioemotional DevelopmenttopakinNo ratings yet
- Mnemonics PDFDocument18 pagesMnemonics PDFEyob Mizan83% (6)
- Growth and DevelopmentDocument47 pagesGrowth and DevelopmentMark Anthony FloresNo ratings yet
- Hypothalamic and Pituitary Drugs (Autosaved)Document41 pagesHypothalamic and Pituitary Drugs (Autosaved)mug ashNo ratings yet
- Changes in Adolescent Bodies and IdentitiesDocument23 pagesChanges in Adolescent Bodies and IdentitiesCath Fofue100% (1)
- Precocious Puberty With Primary Hypothyroidism Due To Autoimmune ThyroiditisDocument3 pagesPrecocious Puberty With Primary Hypothyroidism Due To Autoimmune ThyroiditisShohel RanaNo ratings yet
- Gineco ENGLISHDocument198 pagesGineco ENGLISHVașadi Razvan CristianNo ratings yet
- Language and Communicatio NDocument113 pagesLanguage and Communicatio NLeo MasucolNo ratings yet
- Care of AdolescentDocument32 pagesCare of AdolescentNestor Cabacungan100% (2)
- PcosDocument72 pagesPcosDedy Tesna AmijayaNo ratings yet
- 10 Proven Ways To Get A Deep, Resonant, Authorative VoiceDocument3 pages10 Proven Ways To Get A Deep, Resonant, Authorative Voicearjun100% (1)
- Rites of Passage: Physical, Cognitive Changes in AdolescenceDocument44 pagesRites of Passage: Physical, Cognitive Changes in AdolescenceApple GenesisNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)