You might also like
- MCQ Manual - SCFHSDocument75 pagesMCQ Manual - SCFHSferdinand bolayog0% (3)
- Test Bank For Abnormal Psychology 5th Canadian Edition by BarlowDocument37 pagesTest Bank For Abnormal Psychology 5th Canadian Edition by BarlowNancy Medez100% (37)
- Diagnosis and Management of Gestational Trophoblastic Disease C rat w o ie M ev S R G PODocument56 pagesDiagnosis and Management of Gestational Trophoblastic Disease C rat w o ie M ev S R G PORendy Adhitya PratamaNo ratings yet
- Management of Preterm LaborDocument2 pagesManagement of Preterm LaborpolygoneNo ratings yet
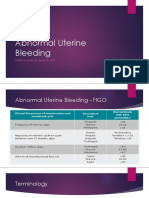
- Abnormal Uterine BleedingDocument33 pagesAbnormal Uterine BleedingGregorius Juan GunawanNo ratings yet
- 12 Friedmans Curve v2Document4 pages12 Friedmans Curve v2Jowi Sal100% (1)
- I. Dystocia: A. CausesDocument9 pagesI. Dystocia: A. CausesDianne GalangNo ratings yet
- M. Preterm and Postterm - NewDocument93 pagesM. Preterm and Postterm - NewRinaNo ratings yet
- Fetal Growth Retardation Assessment and Placental InsufficiencyDocument39 pagesFetal Growth Retardation Assessment and Placental InsufficiencyslyfoxkittyNo ratings yet
- Uterine RuptureDocument21 pagesUterine RuptureSirisha Pemma100% (7)
- Science Investigatory ProjectDocument13 pagesScience Investigatory ProjectSherynhell Ann Perales60% (5)
- Abnormal Uterine BleedingDocument23 pagesAbnormal Uterine BleedingTakeru Ferry100% (1)
- Abnormal Uterine BleedingDocument44 pagesAbnormal Uterine BleedingBezza Mae Roche CruzNo ratings yet
- Aub Updated-1 PDFDocument87 pagesAub Updated-1 PDFEvelyn Pamela Espinoza Morales100% (2)
- Gynecology Abnormal Bleeding 2014aDocument8 pagesGynecology Abnormal Bleeding 2014aBhi-An BatobalonosNo ratings yet
- (SLE) and PregnancyDocument60 pages(SLE) and PregnancyNurfikhaHandayaniNo ratings yet
- GYNE 4.08 Benign and Malignant Lesions of The CervixDocument9 pagesGYNE 4.08 Benign and Malignant Lesions of The CervixGray SnellNo ratings yet
- COMPLETE Medical Disease in PregnancyDocument210 pagesCOMPLETE Medical Disease in PregnancyCHANDREN ARUMUGAMNo ratings yet
- Benign and Malignant Ovarian Tumors (Gynaecology)Document70 pagesBenign and Malignant Ovarian Tumors (Gynaecology)Dr Ali MehdiNo ratings yet
- Abnormal Uterine BleedingDocument7 pagesAbnormal Uterine BleedingBrian Fry100% (1)
- ACOG Abnormal Uterine Bleeding DiagnosisDocument11 pagesACOG Abnormal Uterine Bleeding DiagnosisJimmy Crack CornsNo ratings yet
- Abnormal Uterine BleedingDocument12 pagesAbnormal Uterine BleedingGilang DermawanNo ratings yet
- DystociaDocument6 pagesDystociasarguss14100% (2)
- Obstetrics MnemonicsDocument9 pagesObstetrics MnemonicsJared Khoo Er Hau100% (2)
- Abnormal Uterine BleedingDocument5 pagesAbnormal Uterine Bleedingwuryan dewiNo ratings yet
- 5 - DystociaDocument43 pages5 - DystociaMara Medina - BorleoNo ratings yet
- Comprehensive Guide to Abnormal Uterine Bleeding CausesDocument7 pagesComprehensive Guide to Abnormal Uterine Bleeding CausesRem AlfelorNo ratings yet
- (SLE) and PregnancyDocument39 pages(SLE) and PregnancyRake SardevaNo ratings yet
- Obstetric History and Physical Examination (Ina Irabon)Document49 pagesObstetric History and Physical Examination (Ina Irabon)Benjamin Gabriel100% (1)
- VBACDocument45 pagesVBACJuan Habli SoufalNo ratings yet
- Obstetrics - Operative Vaginal DeliveryDocument5 pagesObstetrics - Operative Vaginal DeliveryJonathanNo ratings yet
- Uterinefibroids 130120064643 Phpapp02Document73 pagesUterinefibroids 130120064643 Phpapp02Tharun KumarNo ratings yet
- Hydramnios and Premature Rupture of MembranesDocument5 pagesHydramnios and Premature Rupture of Membranessarguss14No ratings yet
- Physiological Changes of PregnancyDocument40 pagesPhysiological Changes of PregnancyAita AladianseNo ratings yet
- Planes and Diameters of The PelvisDocument32 pagesPlanes and Diameters of The PelvisRumelle ReyesNo ratings yet
- Ectopic PregnancyDocument5 pagesEctopic PregnancyFaith FuentevillaNo ratings yet
- Abnormal Labor and Dystocia Causes, Evaluation and ManagementDocument63 pagesAbnormal Labor and Dystocia Causes, Evaluation and ManagementJoan LuisNo ratings yet
- Acute Abdomen in PregnancyDocument14 pagesAcute Abdomen in PregnancyNaila WardhanaNo ratings yet
- Ectopic Pregnancy and Abortion: DR - Shamim Rima MBBS, Dmu, FCGP M.PHL, Thesis Part Radiology & ImagimgDocument59 pagesEctopic Pregnancy and Abortion: DR - Shamim Rima MBBS, Dmu, FCGP M.PHL, Thesis Part Radiology & Imagimgdr_shamimrNo ratings yet
- Rcog PpromDocument7 pagesRcog PpromDevi SyamNo ratings yet
- Module 6 - Benign Gynecologic TumorsDocument9 pagesModule 6 - Benign Gynecologic TumorsRenz Francis SasaNo ratings yet
- Φ PathophysiologyDocument4 pagesΦ PathophysiologyMariah AshooriyanNo ratings yet
- Philippine CPG On The Diagnosis and Management of Urinary Tract Infections in Adults-2015 Update - Part 2 PDFDocument140 pagesPhilippine CPG On The Diagnosis and Management of Urinary Tract Infections in Adults-2015 Update - Part 2 PDFspringdingNo ratings yet
- Dr. Sharda Jain: Director: Secretary GeneralDocument91 pagesDr. Sharda Jain: Director: Secretary GeneraljijaniNo ratings yet
- Heart Disease in PregnancyDocument20 pagesHeart Disease in PregnancyAnironOrionNo ratings yet
- OBGYN Revalida Review 2019Document74 pagesOBGYN Revalida Review 2019anonymous100% (1)
- SEIZURE CASE PROTOCOLDocument1 pageSEIZURE CASE PROTOCOLMarco Paulo Reyes NaoeNo ratings yet
- Antiphospholipid Syndrome in Pregnancy: Review of Diagnosis and TreatmentDocument7 pagesAntiphospholipid Syndrome in Pregnancy: Review of Diagnosis and TreatmentDara Dasawulansari SyamsuriNo ratings yet
- Obstetric Gynaecology Jan 11Document32 pagesObstetric Gynaecology Jan 11selvie87No ratings yet
- Benign Gynecologic LesionsDocument103 pagesBenign Gynecologic Lesions201286% (7)
- CPG on Immunization for WomenDocument28 pagesCPG on Immunization for WomenYnoli DiosomitoNo ratings yet
- OSCE Revision OBG DocumentDocument60 pagesOSCE Revision OBG DocumentshreyaNo ratings yet
- Final Ob ChecklistDocument21 pagesFinal Ob ChecklistAlbino Fulgencio Santos III100% (1)
- Uterine ProlapseDocument5 pagesUterine ProlapseAngel de JesusNo ratings yet
- 0.7 Surgery Trans PDFDocument29 pages0.7 Surgery Trans PDFJoy ManzanoNo ratings yet
- Maternal Anatomy OverviewDocument89 pagesMaternal Anatomy OverviewWildelyn JaoNo ratings yet
- SGOP2019 Cervical Cancer GuidelinesDocument8 pagesSGOP2019 Cervical Cancer GuidelinesNico Angelo CopoNo ratings yet
- Uterine ProlapseDocument45 pagesUterine ProlapseAnusree AnusreervNo ratings yet
- Obgyn Clerkship Guide To SuccessDocument6 pagesObgyn Clerkship Guide To SuccessprabhatNo ratings yet
- KEMH Guidelines On Cardiac Disease in PregnancyDocument7 pagesKEMH Guidelines On Cardiac Disease in PregnancyAyesha RazaNo ratings yet
- Pre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Dewhurst's Textbook of Obstetrics & GynaecologyFrom EverandDewhurst's Textbook of Obstetrics & GynaecologyChristoph LeesRating: 2 out of 5 stars2/5 (1)
- Drug Study-AkinetonDocument2 pagesDrug Study-AkinetonKrizia KrizhNo ratings yet
- Complete Blood CountDocument10 pagesComplete Blood CountJohn Lee Lorena Gacusan100% (1)
- Pain Management PDFDocument38 pagesPain Management PDFYulia Fransisca PurbaNo ratings yet
- BDI-II and BAI ReviewDocument3 pagesBDI-II and BAI ReviewMary Winston DozierNo ratings yet
- Transmittal New FormatDocument7 pagesTransmittal New FormatRheymark Ramada ButronNo ratings yet
- SpirulinaDocument57 pagesSpirulinaMarcus Gibson100% (4)
- MSDS Ponceau SXDocument4 pagesMSDS Ponceau SXArthur Reynaldo DevicoNo ratings yet
- Anantara Family Medicine QuestionsDocument53 pagesAnantara Family Medicine QuestionsMochamadAriWibowoNo ratings yet
- Factsheet: Low Libido (Sexual Desire)Document1 pageFactsheet: Low Libido (Sexual Desire)vdphbfiuNo ratings yet
- Editorial Letter: ﺪﻠﺠﻣ 1 دﺪﻋ 3 - 2004 - Volume 1-N°3, 2004Document141 pagesEditorial Letter: ﺪﻠﺠﻣ 1 دﺪﻋ 3 - 2004 - Volume 1-N°3, 2004CH Karim100% (1)
- HSRCDocument53 pagesHSRCAbhishek Kumar SharmaNo ratings yet
- Tracheostomy Guide: Procedures, Indications, Advantages & RisksDocument31 pagesTracheostomy Guide: Procedures, Indications, Advantages & RisksHari PranotoNo ratings yet
- Deep Vein ThrombosisDocument16 pagesDeep Vein ThrombosisHarinesh JayNo ratings yet
- Stages of HivDocument4 pagesStages of Hivapi-273431943No ratings yet
- ThePaleoApproach List of Autoimmune DiseasesDocument3 pagesThePaleoApproach List of Autoimmune DiseasesdevabakhtiNo ratings yet
- Caregiver Stress and The Patient With Dementia Continuum 2016Document7 pagesCaregiver Stress and The Patient With Dementia Continuum 2016Habib G. Moutran BarrosoNo ratings yet
- Case Study and Research On EMDR For Combat PTSDDocument21 pagesCase Study and Research On EMDR For Combat PTSDDaniel R. Gaita, MA, LMSWNo ratings yet
- Nursing Intervention Plan for Fracture PatientDocument2 pagesNursing Intervention Plan for Fracture PatientAce Dioso TubascoNo ratings yet
- Complete Report of Introduction Biotechnology: "Tempe Making (Soybean Cake) "Document21 pagesComplete Report of Introduction Biotechnology: "Tempe Making (Soybean Cake) "1123khaliqNo ratings yet
- Ultrasound SonographyDocument3 pagesUltrasound SonographyBinta BaptisteNo ratings yet
- Parkinson's UK Lincoln Branch News July 2017Document6 pagesParkinson's UK Lincoln Branch News July 2017daniel2bratleyNo ratings yet
- Dental List of Specialties Registration StandardDocument3 pagesDental List of Specialties Registration StandardJose PerezNo ratings yet
- Diagnosis, Conceptualization and Treatment Planning For AdultsDocument350 pagesDiagnosis, Conceptualization and Treatment Planning For AdultsFelipe Orejuela SotoNo ratings yet
- Perioperative Cardiac Arrest in The Operating Room Environment A Review MinervAnest 2017Document9 pagesPerioperative Cardiac Arrest in The Operating Room Environment A Review MinervAnest 2017RicardoNo ratings yet
- Positive Mental Health Assignment Report 2018Document6 pagesPositive Mental Health Assignment Report 2018api-404544260No ratings yet
- Drug StudyDocument10 pagesDrug StudyRye IbarraNo ratings yet
- The Ultimate Synergy Against Cancer: Fucoidan and AHCCDocument98 pagesThe Ultimate Synergy Against Cancer: Fucoidan and AHCCDr. Susana Trujillo100% (2)