You might also like
- Nursing Care PlanDocument31 pagesNursing Care PlanStephen Paul100% (2)
- Full Report Interventions For Children On The Autism Spectrum A Synthesis of Research EvidenceDocument503 pagesFull Report Interventions For Children On The Autism Spectrum A Synthesis of Research EvidenceGiedrė Skaisgirytė100% (1)
- History of PsychotherapyDocument21 pagesHistory of PsychotherapypamNo ratings yet
- Hair Like A FoxDocument79 pagesHair Like A FoxDiego Caban100% (1)
- Presentation On: Automated Database: By: Binu Thapa Binita Rupakheti Aayusma PradhanDocument31 pagesPresentation On: Automated Database: By: Binu Thapa Binita Rupakheti Aayusma PradhanbimuNo ratings yet
- Infection in Knee ReplacementDocument358 pagesInfection in Knee Replacementorthofitness2017100% (1)
- E-1-Osteoporosis and Periodontitis 2016Document14 pagesE-1-Osteoporosis and Periodontitis 2016Yessid Baltazar Arango100% (1)
- AIRP Vol 2Document735 pagesAIRP Vol 2djarcos100% (1)
- SBAR ReferenceDocument16 pagesSBAR ReferenceTni JolieNo ratings yet
- The Osteoporotic Syndrome: Detection, Prevention, and TreatmentFrom EverandThe Osteoporotic Syndrome: Detection, Prevention, and TreatmentNo ratings yet
- Bone Reports: A A B C C B CDocument9 pagesBone Reports: A A B C C B Caeroforce20No ratings yet
- Cia 15 485Document7 pagesCia 15 485Faradilla PuspitasariNo ratings yet
- Tie Ppo Franci o 2017Document9 pagesTie Ppo Franci o 2017Deddy RifkiNo ratings yet
- Clinical Presentation, Management, and Prognosis of Pseudogout in Joint Arthroplasty: A Retrospective Cohort StudyDocument7 pagesClinical Presentation, Management, and Prognosis of Pseudogout in Joint Arthroplasty: A Retrospective Cohort StudyPutri Aswariyah RamliNo ratings yet
- Proximal Femur Fractures. Definition, Epidemiology, Anatomy, BiomechanicsDocument7 pagesProximal Femur Fractures. Definition, Epidemiology, Anatomy, BiomechanicsConstantin VascautanNo ratings yet
- F. Lapi, M. Simonetti, R. Michieli, A. Pasqua, M.L. Brandi, B. Frediani, C. Cricelli, G. MazzagliaDocument6 pagesF. Lapi, M. Simonetti, R. Michieli, A. Pasqua, M.L. Brandi, B. Frediani, C. Cricelli, G. Mazzagliafirdha afghaniNo ratings yet
- 1 s2.0 S8756328217302302 MainDocument6 pages1 s2.0 S8756328217302302 Mainahmed fikryNo ratings yet
- Osteoporosis and Sarcopenia: Hiroshi Hagino, Takashi WadaDocument4 pagesOsteoporosis and Sarcopenia: Hiroshi Hagino, Takashi WadaAdit DaniNo ratings yet
- Pharmacotherapy of OsteoporosisDocument7 pagesPharmacotherapy of OsteoporosisFlorentina NadisaNo ratings yet
- OsteopeniaDocument9 pagesOsteopeniaMohamed EssallaaNo ratings yet
- Dhanwal DK2011Document9 pagesDhanwal DK2011M MNo ratings yet
- The Ligament Injury Connection To Osteoarthritis: Wonder Why?Document11 pagesThe Ligament Injury Connection To Osteoarthritis: Wonder Why?Saifuddin HaswareNo ratings yet
- Management of Severe OsteoporosisDocument16 pagesManagement of Severe OsteoporosisZendy Nicole Cano SaavedraNo ratings yet
- FulltextDocument11 pagesFulltextajeet84bhu2920No ratings yet
- Osteoporosis Prevention, Diagnosis, and Therapy: Consensus ConferenceDocument11 pagesOsteoporosis Prevention, Diagnosis, and Therapy: Consensus ConferenceCorin Boice TelloNo ratings yet
- Representation To The Accident and Emergency Department Within 1-Year of A Fractured Neck of FemurDocument5 pagesRepresentation To The Accident and Emergency Department Within 1-Year of A Fractured Neck of FemurOgirahma T. NaidNo ratings yet
- Total Knee Replacement Surgery TKR IndiaDocument3 pagesTotal Knee Replacement Surgery TKR IndiaAnonymous x8fY69CrnNo ratings yet
- Assessment of Fracture Risk and Its Application To Screening For Postmenopausal Osteoporosis Synopsis of A WHO ReportDocument14 pagesAssessment of Fracture Risk and Its Application To Screening For Postmenopausal Osteoporosis Synopsis of A WHO ReportKhủngLongSiêuNguyHiểmNo ratings yet
- A Perspective On Osteoarthritis Research in Singapore: ReviewDocument9 pagesA Perspective On Osteoarthritis Research in Singapore: ReviewRhinaNo ratings yet
- Arthroplasty TodayDocument5 pagesArthroplasty TodayTya VenyNo ratings yet
- Bone Fragility Fractures in CKD PatientsDocument12 pagesBone Fragility Fractures in CKD PatientsPawan MishraNo ratings yet
- Systemic Diseases and Medications InfluenceDocument20 pagesSystemic Diseases and Medications InfluencealinagaxiolaariasNo ratings yet
- International Journal of Orthopaedic and Trauma NursingDocument8 pagesInternational Journal of Orthopaedic and Trauma NursingSaugi HudaNo ratings yet
- Global, Regional Prevalence, Incidence and Risk Factors of Knee Osteoarthritis PopulationDocument13 pagesGlobal, Regional Prevalence, Incidence and Risk Factors of Knee Osteoarthritis PopulationnurjannahnasirNo ratings yet
- Osteoarthritis 1 13 2 3 2x: Musculoskeletal FactsheetsDocument2 pagesOsteoarthritis 1 13 2 3 2x: Musculoskeletal Factsheetsfidatahir93No ratings yet
- J of Bone Mineral Res - 2016 - Khosla - A Crisis in The Treatment of OsteoporosisDocument3 pagesJ of Bone Mineral Res - 2016 - Khosla - A Crisis in The Treatment of OsteoporosisFerdinan ChristianNo ratings yet
- Reaching A BetterDocument6 pagesReaching A BetterAdyas AdrianaNo ratings yet
- Geriatria y OrtopediaDocument28 pagesGeriatria y OrtopediaHector VallejosNo ratings yet
- Impact of Bisphosphonates and Comorbidities On Initial Hip Fracture PrognosisDocument9 pagesImpact of Bisphosphonates and Comorbidities On Initial Hip Fracture PrognosisDavids MarinNo ratings yet
- Dioguardi, 2023Document20 pagesDioguardi, 2023Aneliza de Fatima Moraes da SilvaNo ratings yet
- MathematicsDocument20 pagesMathematicsoscarNo ratings yet
- Bone Reports: Case ReportDocument8 pagesBone Reports: Case ReportDaniella NúñezNo ratings yet
- 3 Minute DFU ExamDocument6 pages3 Minute DFU ExamRinky MansukhaniNo ratings yet
- 2 OaDocument11 pages2 OaNitya KrishnaNo ratings yet
- Epidemiology and Patho-Anatomical Pattern of 2,011 Humeral Fractures: Data From The Swedish Fracture RegisterDocument10 pagesEpidemiology and Patho-Anatomical Pattern of 2,011 Humeral Fractures: Data From The Swedish Fracture RegisterGabriel GolesteanuNo ratings yet
- Chambrone2016 ONM2Document5 pagesChambrone2016 ONM2drjaviervaldezNo ratings yet
- Overview of Epidemiology: Rockwood & Green's Fractures in Adults, 6th EditionDocument53 pagesOverview of Epidemiology: Rockwood & Green's Fractures in Adults, 6th EditionSilvia TacheNo ratings yet
- 1 s2.0 S094096021830089X MainDocument8 pages1 s2.0 S094096021830089X MainDANTE DELEGUERYNo ratings yet
- Risk Factors and Burden of Osteoarthritis: SciencedirectDocument5 pagesRisk Factors and Burden of Osteoarthritis: SciencedirectlindapramusintaNo ratings yet
- J of Bone Mineral Res - 2022 - Kjeldgaard - Impact of Total Hip Replacements On The Incidence of Hip Fractures in NorwayDocument8 pagesJ of Bone Mineral Res - 2022 - Kjeldgaard - Impact of Total Hip Replacements On The Incidence of Hip Fractures in NorwayStefano RobertoNo ratings yet
- The Diamond Concept' For Long Bone Non-Union Management: Journal of Orthopaedics and TraumatologyDocument13 pagesThe Diamond Concept' For Long Bone Non-Union Management: Journal of Orthopaedics and TraumatologyFarizka Dwinda HNo ratings yet
- International Journal of Health Sciences and Research: Osteoporosis-Do We Need To Think Beyond Bone Mineral Density?Document5 pagesInternational Journal of Health Sciences and Research: Osteoporosis-Do We Need To Think Beyond Bone Mineral Density?Ahmad Ghozi Al AkhmarNo ratings yet
- 1 s2.0 S1530891X20481868 MainDocument9 pages1 s2.0 S1530891X20481868 MainSaugi HudaNo ratings yet
- Comparison of Effectiveness and Safety of Ibandronate and Mi - 2017 - OsteoporosDocument8 pagesComparison of Effectiveness and Safety of Ibandronate and Mi - 2017 - OsteoporosDavid Ruiz GonzalezNo ratings yet
- Hip and Knee Replacement 1: SeriesDocument10 pagesHip and Knee Replacement 1: SeriesF CPNo ratings yet
- Implants in Medically Compromised PatientsDocument12 pagesImplants in Medically Compromised PatientsShreyans DamadeNo ratings yet
- Critical Reviews in Oncology / Hematology: H Elios Bertin, A. Gomez-Brouchet, F. R EdiniDocument9 pagesCritical Reviews in Oncology / Hematology: H Elios Bertin, A. Gomez-Brouchet, F. R EdiniHagar AlaaNo ratings yet
- Guidelines For Diagnosis and Management of OsteoporosisDocument17 pagesGuidelines For Diagnosis and Management of OsteoporosisVanessaCockerNo ratings yet
- Osteoporosis y COVID19 InglesDocument5 pagesOsteoporosis y COVID19 Inglescesar kevin lopez marquezNo ratings yet
- InTech-Knee Pain in Adults Adolescents Diagnosis and TreatmentDocument32 pagesInTech-Knee Pain in Adults Adolescents Diagnosis and Treatmentevil freakNo ratings yet
- Journal of Clinical & Translational EndocrinologyDocument6 pagesJournal of Clinical & Translational EndocrinologyEka JuliantaraNo ratings yet
- Global Burden of Severe Periodontitis in 1990-2010: A Systematic Review and Meta-RegressionDocument10 pagesGlobal Burden of Severe Periodontitis in 1990-2010: A Systematic Review and Meta-RegressionRaul CamargoNo ratings yet
- Proximal Humerus Fractures Epidemiology and TrendsDocument5 pagesProximal Humerus Fractures Epidemiology and TrendsHelena Sofia Fonseca Paiva De Sousa TelesNo ratings yet
- The Effect of Body Mass Index On Components Size in Patients With Total Knee ReplacementDocument5 pagesThe Effect of Body Mass Index On Components Size in Patients With Total Knee ReplacementalirezanouriNo ratings yet
- KneeDocument10 pagesKneeMario Rico GonzálezNo ratings yet
- Archives of Osteoporosis, 2021, 16, 102 - The Indian Society For Bone and Mineral Research (ISBMR) Position Statement For The DiagnosisDocument13 pagesArchives of Osteoporosis, 2021, 16, 102 - The Indian Society For Bone and Mineral Research (ISBMR) Position Statement For The DiagnosisBHUENDOCRINE SRNo ratings yet
- Injury: Pasi P. Rinne, Minna K. Laitinen, Tuomas Huttunen, Pekka Kannus, Ville M. MattilaDocument5 pagesInjury: Pasi P. Rinne, Minna K. Laitinen, Tuomas Huttunen, Pekka Kannus, Ville M. MattilajavierjaracanovasNo ratings yet
- International Journal of Orthopaedic and Trauma NursingDocument8 pagesInternational Journal of Orthopaedic and Trauma NursingSaugi HudaNo ratings yet
- International Journal of Surgery OpenDocument11 pagesInternational Journal of Surgery OpenSaugi HudaNo ratings yet
- 1 s2.0 S1530891X20481868 MainDocument9 pages1 s2.0 S1530891X20481868 MainSaugi HudaNo ratings yet
- Chinese Journal of Traumatology: Sen Yang, Yi-Jie Liu, Wei-Min JiangDocument6 pagesChinese Journal of Traumatology: Sen Yang, Yi-Jie Liu, Wei-Min JiangSaugi HudaNo ratings yet
- 1 s2.0 S0020138320303521 MainDocument8 pages1 s2.0 S0020138320303521 MainSaugi HudaNo ratings yet
- Electrotherapy and Tissue RepairDocument20 pagesElectrotherapy and Tissue RepairNguyen ThuanNo ratings yet
- Covid-19 Human Igm/Igg Rapid Test: Intended UseDocument3 pagesCovid-19 Human Igm/Igg Rapid Test: Intended UseArijit DebNo ratings yet
- Fistula in Ano Final For PresentationDocument41 pagesFistula in Ano Final For PresentationRhajeeb Aennas SugalaNo ratings yet
- FCPS II Nephrology Clinical and VivaDocument2 pagesFCPS II Nephrology Clinical and Vivateena6506763No ratings yet
- DJK It's Just A Concussion NoteDocument40 pagesDJK It's Just A Concussion NoteVibhav SinghNo ratings yet
- What's Covered? Extra Details: Your Choice ExtrasDocument3 pagesWhat's Covered? Extra Details: Your Choice ExtrasNietharshan EapenNo ratings yet
- Bahan Kemas - Selisih SO Vs Sistem FY2020 - 291220Document17 pagesBahan Kemas - Selisih SO Vs Sistem FY2020 - 291220Idan RidwanNo ratings yet
- Top 200 Pharmaceuticals 2021V2Document1 pageTop 200 Pharmaceuticals 2021V2Amin AminiradNo ratings yet
- Susruthasamhitha Part 3Document42 pagesSusruthasamhitha Part 3Suvarna NalapatNo ratings yet
- 2020 Article 5890Document779 pages2020 Article 5890desa jotonNo ratings yet
- Concepts of Prevention and Control of Diseases: R. VenkitachalamDocument75 pagesConcepts of Prevention and Control of Diseases: R. Venkitachalamtomzki007No ratings yet
- Pharmacology Chapter 3 and 4Document2 pagesPharmacology Chapter 3 and 4Dingal AijayNo ratings yet
- Diagnosis and Management of Placenta PreviaDocument6 pagesDiagnosis and Management of Placenta PreviaNoveno Semestre FmuaqNo ratings yet
- ERAS Perioperative Care in Lumbar Spine FusionDocument24 pagesERAS Perioperative Care in Lumbar Spine FusionDionisius RiantoNo ratings yet
- PresbikusisDocument7 pagesPresbikusisLuluk AisyahNo ratings yet
- Malignant Hypertension - Dr. Todung PDFDocument12 pagesMalignant Hypertension - Dr. Todung PDFMuhammad Khoirul SodiqNo ratings yet
- Causes of Cataracts in DogsDocument2 pagesCauses of Cataracts in DogsBibek SutradharNo ratings yet
- Super Arrow Flex Sheath - Brochure - EN PDFDocument3 pagesSuper Arrow Flex Sheath - Brochure - EN PDFbiomedical_com_brNo ratings yet
- A Guide: Christian Medical CollegeDocument75 pagesA Guide: Christian Medical CollegeSanjay Kumar SekhardeoNo ratings yet
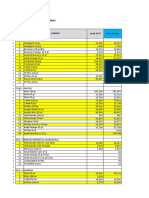
- Stokopname Poliklinik Ibnu Sina Balikpapan Unit: URD SepingganDocument24 pagesStokopname Poliklinik Ibnu Sina Balikpapan Unit: URD SepingganPelangi Cahya Ratu DoraNo ratings yet
- Kursk State Medical UniversityDocument19 pagesKursk State Medical UniversitydevilstNo ratings yet
- MsgenitourinaryDocument7 pagesMsgenitourinarybekbekk cabahugNo ratings yet
- 21 Iajps21102017 PDFDocument9 pages21 Iajps21102017 PDFBaru Chandrasekhar RaoNo ratings yet