You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Risk Assessment TemplateDocument3 pagesRisk Assessment TemplateGus VanGeijtenbeekNo ratings yet
- The Procedure: Cleaning ValidationDocument4 pagesThe Procedure: Cleaning ValidationYousif100% (1)
- PMS SopDocument8 pagesPMS Sopstevekent40% (5)
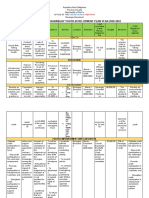
- Comprehensive Barangay Youth Development Plan Year 2020-2022Document7 pagesComprehensive Barangay Youth Development Plan Year 2020-2022ralf100% (1)
- Organization TheoryDocument110 pagesOrganization TheoryOhi OyakhireNo ratings yet
- Chapter 25Document63 pagesChapter 25Jœnríčk AzueloNo ratings yet
- STUDY MANUAL Planning Your Career in Business (V3)Document56 pagesSTUDY MANUAL Planning Your Career in Business (V3)Cristina IsbășescuNo ratings yet
- Hydroxychloroquine-Induced Retinal Toxicity: Ophthalmic PearlsDocument3 pagesHydroxychloroquine-Induced Retinal Toxicity: Ophthalmic PearlsYasminSolbergNo ratings yet
- Eyes On A Cure: Patients & Caregiver Symposium: April 5-7, 2019Document50 pagesEyes On A Cure: Patients & Caregiver Symposium: April 5-7, 2019YasminSolbergNo ratings yet
- Normal Findings and Complications of Breast Implants.: Poster No.: Congress: Type: AuthorsDocument35 pagesNormal Findings and Complications of Breast Implants.: Poster No.: Congress: Type: AuthorsYasminSolbergNo ratings yet
- Um DEDocument68 pagesUm DEYasminSolbergNo ratings yet
- Optical Coherence Tomography Angiography Findings in Stargardt DiseaseDocument11 pagesOptical Coherence Tomography Angiography Findings in Stargardt DiseaseYasminSolbergNo ratings yet
- Mackpro WLW1Document1 pageMackpro WLW1Saeed AhmedNo ratings yet
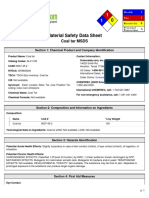
- Msds Coal PDFDocument5 pagesMsds Coal PDFWinaNo ratings yet
- The Effect of Cholecystectomy On The Lipid Profile of Patients With Gallstone Disease: A Prospective StudyDocument5 pagesThe Effect of Cholecystectomy On The Lipid Profile of Patients With Gallstone Disease: A Prospective StudyMia AmeliaNo ratings yet
- HRS - Integrated - Contract - and - Handbook - v2 - 2020 - UpdateDocument6 pagesHRS - Integrated - Contract - and - Handbook - v2 - 2020 - UpdateCamilo ZapataNo ratings yet
- Alcohol AbuseDocument2 pagesAlcohol AbuseShanice OrtizNo ratings yet
- Resisted ExerciseDocument53 pagesResisted ExerciseEliud MbuteNo ratings yet
- Medicolegal Aspects of Hurt Injury and WoundDocument6 pagesMedicolegal Aspects of Hurt Injury and WoundSebin JamesNo ratings yet
- Dis-Infection With Ozone SystemDocument6 pagesDis-Infection With Ozone SystemSwaminathan ThayumanavanNo ratings yet
- Floyd CVDocument10 pagesFloyd CVKristy MayNo ratings yet
- Correct Myth and Fallacies About NonDocument2 pagesCorrect Myth and Fallacies About NonRhuj's DiaryNo ratings yet
- The Impact of Exercise Therapy and Abdominal Binding in The Management of Diastasis Recti Abdominis in The Early Post-Partum Period: A Pilot Randomized Controlled TrialDocument17 pagesThe Impact of Exercise Therapy and Abdominal Binding in The Management of Diastasis Recti Abdominis in The Early Post-Partum Period: A Pilot Randomized Controlled TrialSara EmmanuelaNo ratings yet
- Biochem Metab PacopDocument9 pagesBiochem Metab PacopJifelNo ratings yet
- G10 Sip Primer PDFDocument18 pagesG10 Sip Primer PDFVincent Hiram LoricoNo ratings yet
- Reading Test 3Document10 pagesReading Test 3Tuyết NhưNo ratings yet
- E Tech Consultant (Introduction Profile)Document10 pagesE Tech Consultant (Introduction Profile)E Tech ConsultantNo ratings yet
- Bruce TuckmanDocument1 pageBruce TuckmanFlorin AstileanNo ratings yet
- Epocast 1628 BDocument10 pagesEpocast 1628 BNICKYNo ratings yet
- NOV. 2 - 6@ENGLISH 9 Learner Activity Sheet (LAS)Document4 pagesNOV. 2 - 6@ENGLISH 9 Learner Activity Sheet (LAS)Maria BuizonNo ratings yet
- Elliott 2011Document12 pagesElliott 2011oscar eduardo mateus ariasNo ratings yet
- Health Aging and The Top 10 Things To Ask - Dr.-William-DalzielDocument54 pagesHealth Aging and The Top 10 Things To Ask - Dr.-William-DalzielJason WongNo ratings yet
- State of New South Wales V WilmotDocument40 pagesState of New South Wales V WilmotToby VueNo ratings yet
- Broth For BifidobacteriumDocument2 pagesBroth For BifidobacteriumAhnaph RafinNo ratings yet
- EmergingTech AppsDocument25 pagesEmergingTech AppsMahmoud Abdelfatah MahgoubNo ratings yet