You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Pioneer MVH-S21BT - S215BT - S219BT CRT6291Document26 pagesPioneer MVH-S21BT - S215BT - S219BT CRT6291corelc89% (9)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Camouflage Yourself and Individual EquipmentDocument16 pagesCamouflage Yourself and Individual EquipmentInficeman100% (1)
- JTlecture 01 PrintDocument17 pagesJTlecture 01 PrintJae-Soo ChangNo ratings yet
- Men's Prints & Graphics Forecast A/W 23/24: Care CultureDocument17 pagesMen's Prints & Graphics Forecast A/W 23/24: Care CultureAKSHAY NATHNo ratings yet
- Characterization and Toxicity of Temulawak Curcuminoid NanoparticlesDocument11 pagesCharacterization and Toxicity of Temulawak Curcuminoid NanoparticlesFathnurainiNo ratings yet
- Jurnal Ilmiah KefarmasianDocument9 pagesJurnal Ilmiah KefarmasianFathnurainiNo ratings yet
- GSM Genitourinary Syndrome of Menopause Why Should We CareDocument5 pagesGSM Genitourinary Syndrome of Menopause Why Should We CareFathnurainiNo ratings yet
- Terdapat Hubungan Kadar Estradiol Dengan Ekspresi Kolagen Dan Elastin Pada Vagina Premenopause Dan PascamenopauseDocument6 pagesTerdapat Hubungan Kadar Estradiol Dengan Ekspresi Kolagen Dan Elastin Pada Vagina Premenopause Dan PascamenopauseFathnurainiNo ratings yet
- FluidDocument4 pagesFluidt5qhpc2ck9No ratings yet
- Installation and Operation Manual: 14,000 Pound Capacity Commercial Grade Four-Post Lifts Models: HD-14TDocument52 pagesInstallation and Operation Manual: 14,000 Pound Capacity Commercial Grade Four-Post Lifts Models: HD-14TLê Xuân SangNo ratings yet
- SATIP-P-104-10 Rev 7 FinalDocument2 pagesSATIP-P-104-10 Rev 7 FinalHatemS.MashaGbeh0% (1)
- Medical MnemonicsDocument107 pagesMedical MnemonicsdrabuelaNo ratings yet
- Illustrated Parts List: Ta-C84 For Solaris Urbino 12H November 2011Document24 pagesIllustrated Parts List: Ta-C84 For Solaris Urbino 12H November 2011Leszek MarczakNo ratings yet
- Intel® Core™ I3-9100f Processor (6M Cache, Up To 4.20 GHZ) Specificatii Tehnice CompatibilitatiDocument3 pagesIntel® Core™ I3-9100f Processor (6M Cache, Up To 4.20 GHZ) Specificatii Tehnice CompatibilitatiNicu MuțNo ratings yet
- List of Participants - WorkshopDocument5 pagesList of Participants - WorkshopSven del PinoNo ratings yet
- Eden For Grown-Ups: Toward A New Ethic of Earth, of Sex, and of CreationDocument7 pagesEden For Grown-Ups: Toward A New Ethic of Earth, of Sex, and of CreationNYU Press86% (7)
- Heron of Alexandria-Math Contributions-Square Root Method and Area of A TriangleDocument11 pagesHeron of Alexandria-Math Contributions-Square Root Method and Area of A TriangleDr Srinivasan Nenmeli -KNo ratings yet
- For Current Affairs January 2Document37 pagesFor Current Affairs January 210I42 Yash shethNo ratings yet
- Basic Principles of Chemistry PracticalsDocument41 pagesBasic Principles of Chemistry PracticalsMufaro NyamutoraNo ratings yet
- (June 2011) CAS 100 Informative Speech #2 - Technology Meets FashionDocument3 pages(June 2011) CAS 100 Informative Speech #2 - Technology Meets FashionLaura Wake-RamosNo ratings yet
- UPS CalculatorDocument1 pageUPS CalculatordesignselvaNo ratings yet
- State Space Models: (Valid For Any Nonlinear Causal System)Document59 pagesState Space Models: (Valid For Any Nonlinear Causal System)Anonymous HsoXPyNo ratings yet
- 6 Halaba Bridge PierDocument79 pages6 Halaba Bridge PierReader of Down HillNo ratings yet
- CE Refresher Nov 2022 - Tuzon - Set 7 F2FDocument2 pagesCE Refresher Nov 2022 - Tuzon - Set 7 F2Femielyn lafortezaNo ratings yet
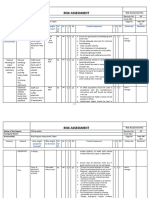
- RA-05-Office SafetyDocument5 pagesRA-05-Office Safetyamritha n krishnaNo ratings yet
- Gujarat SG ReportDocument544 pagesGujarat SG ReporthareshNo ratings yet
- ESM TG Movement BitbankDocument55 pagesESM TG Movement BitbankSandeepNo ratings yet
- Full Synthetic Motor OilDocument1 pageFull Synthetic Motor OilfghdNo ratings yet
- Common ENT 1 Hearing LossDocument24 pagesCommon ENT 1 Hearing LossBalakrishnan DoraisamiNo ratings yet
- Exercise 1 - TVM & Equivalence 2.0Document5 pagesExercise 1 - TVM & Equivalence 2.0Bayu PurnamaNo ratings yet
- 16 MM XA Series & 22 MM XW Series Emergency Stop SwitchesDocument20 pages16 MM XA Series & 22 MM XW Series Emergency Stop SwitchesMuhamad PriyatnaNo ratings yet
- Minor Project Phase-1 List of Supervisors & Titles AY 21-22Document5 pagesMinor Project Phase-1 List of Supervisors & Titles AY 21-22ASHISH KUMAR KEWAT Vel Tech, ChennaiNo ratings yet
- Types of Studies - NRC Research Institute (FDA)Document3 pagesTypes of Studies - NRC Research Institute (FDA)Muhammad ReyhanNo ratings yet
- Pilot Checklist CompleteDocument123 pagesPilot Checklist CompletetachelmemoriesNo ratings yet