You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CSEC Jan 2011 Paper 1Document8 pagesCSEC Jan 2011 Paper 1R.D. KhanNo ratings yet
- General Diesel Engine Diagnostic Guide PDFDocument3 pagesGeneral Diesel Engine Diagnostic Guide PDFan0th3r_0n3No ratings yet
- Perkins 20 Kva (404D-22G)Document2 pagesPerkins 20 Kva (404D-22G)RavaelNo ratings yet
- Guide To Growing MangoDocument8 pagesGuide To Growing MangoRhenn Las100% (2)
- Hotel ManagementDocument34 pagesHotel ManagementGurlagan Sher GillNo ratings yet
- Recall, Initiative and ReferendumDocument37 pagesRecall, Initiative and ReferendumPhaura Reinz100% (1)
- Marine Lifting and Lashing HandbookDocument96 pagesMarine Lifting and Lashing HandbookAmrit Raja100% (1)
- Wind Energy in MalaysiaDocument17 pagesWind Energy in MalaysiaJia Le ChowNo ratings yet
- Daraman vs. DENRDocument2 pagesDaraman vs. DENRJeng GacalNo ratings yet
- Case PBL ICM2 Week 3 Jumat-TSDocument33 pagesCase PBL ICM2 Week 3 Jumat-TSsylvia haryantoNo ratings yet
- Case ICM II MONDAY Week 2 - TSDocument24 pagesCase ICM II MONDAY Week 2 - TSsylvia haryantoNo ratings yet
- PBL 1-1 CFSDocument54 pagesPBL 1-1 CFSsylvia haryantoNo ratings yet
- Technique of The Dermatologic Physical Examination: DiasDocument6 pagesTechnique of The Dermatologic Physical Examination: Diassylvia haryantoNo ratings yet
- Revisi (2) Jadwal Hemato 2021Document3 pagesRevisi (2) Jadwal Hemato 2021sylvia haryantoNo ratings yet
- Treatment of Anemia - No VidDocument69 pagesTreatment of Anemia - No Vidsylvia haryantoNo ratings yet
- How To Interpret HEMATOLOGY Test ResultsDocument36 pagesHow To Interpret HEMATOLOGY Test Resultssylvia haryantoNo ratings yet
- CS321 Computer ArchitectureDocument160 pagesCS321 Computer ArchitectureAnurag kumarNo ratings yet
- Resume Jameel 22Document3 pagesResume Jameel 22sandeep sandyNo ratings yet
- Online Learning Interactions During The Level I Covid-19 Pandemic Community Activity Restriction: What Are The Important Determinants and Complaints?Document16 pagesOnline Learning Interactions During The Level I Covid-19 Pandemic Community Activity Restriction: What Are The Important Determinants and Complaints?Maulana Adhi Setyo NugrohoNo ratings yet
- M J 1 MergedDocument269 pagesM J 1 MergedsanyaNo ratings yet
- Ss 7 Unit 2 and 3 French and British in North AmericaDocument147 pagesSs 7 Unit 2 and 3 French and British in North Americaapi-530453982No ratings yet
- Role of The Government in HealthDocument6 pagesRole of The Government in Healthptv7105No ratings yet
- Rating SheetDocument3 pagesRating SheetShirwin OliverioNo ratings yet
- Himachal Pradesh Important NumbersDocument3 pagesHimachal Pradesh Important NumbersRaghav RahinwalNo ratings yet
- Multispan LC 2046 Length Counter PDFDocument2 pagesMultispan LC 2046 Length Counter PDFvinod kumarNo ratings yet
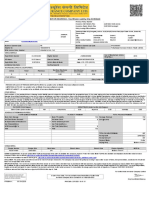
- MOTOR INSURANCE - Two Wheeler Liability Only SCHEDULEDocument1 pageMOTOR INSURANCE - Two Wheeler Liability Only SCHEDULESuhail V VNo ratings yet
- Using Boss Tone Studio For Me-25Document4 pagesUsing Boss Tone Studio For Me-25Oskar WojciechowskiNo ratings yet
- Course Specifications: Fire Investigation and Failure Analysis (E901313)Document2 pagesCourse Specifications: Fire Investigation and Failure Analysis (E901313)danateoNo ratings yet
- DC Servo MotorDocument6 pagesDC Servo MotortaindiNo ratings yet
- ICSI-Admit-Card (1) - 230531 - 163936Document17 pagesICSI-Admit-Card (1) - 230531 - 163936SanjayNo ratings yet
- Manual 40ku6092Document228 pagesManual 40ku6092Marius Stefan BerindeNo ratings yet
- Web Technology PDFDocument3 pagesWeb Technology PDFRahul Sachdeva100% (1)
- Case Assignment 2Document5 pagesCase Assignment 2Ashish BhanotNo ratings yet
- Microwave Drying of Gelatin Membranes and Dried Product Properties CharacterizationDocument28 pagesMicrowave Drying of Gelatin Membranes and Dried Product Properties CharacterizationDominico Delven YapinskiNo ratings yet
- Employees' Pension Scheme, 1995: Form No. 10 C (E.P.S)Document4 pagesEmployees' Pension Scheme, 1995: Form No. 10 C (E.P.S)nasir ahmedNo ratings yet
- Appendix - 5 (Under The Bye-Law No. 19 (B) )Document3 pagesAppendix - 5 (Under The Bye-Law No. 19 (B) )jytj1No ratings yet
- Labstan 1Document2 pagesLabstan 1Samuel WalshNo ratings yet