You might also like
- The Care Process: Assessment, planning, implementation and evaluation in healthcareFrom EverandThe Care Process: Assessment, planning, implementation and evaluation in healthcareNo ratings yet
- ReportDocument126 pagesReportNeha Roy100% (1)
- Overcoming Selective Blindness: Improving Services from the Bedside to the Boardroom and BeyondFrom EverandOvercoming Selective Blindness: Improving Services from the Bedside to the Boardroom and BeyondNo ratings yet
- Sip Mouni & Gopi 18Document47 pagesSip Mouni & Gopi 18Anonymous XrN5ZaHtMNo ratings yet
- Care For Vulnerable Populations During COVID-19 PandemicFrom EverandCare For Vulnerable Populations During COVID-19 PandemicNo ratings yet
- Fit For The Future A Vision For General Prac Ce : #FuturevisiongpDocument53 pagesFit For The Future A Vision For General Prac Ce : #FuturevisiongpJohn SMithNo ratings yet
- A Handbook for Student Nurses, 201819 edition: Introducing key issues relevant for practiceFrom EverandA Handbook for Student Nurses, 201819 edition: Introducing key issues relevant for practiceNo ratings yet
- MGT 2Document1,042 pagesMGT 2kavi kandhuNo ratings yet
- Priyanshu - Sarkar - Project Report On Internship ProgramDocument25 pagesPriyanshu - Sarkar - Project Report On Internship ProgramLog InNo ratings yet
- Organizing Nursing Services and Patient CareDocument31 pagesOrganizing Nursing Services and Patient CarejessyNo ratings yet
- Nebat ToffikDocument42 pagesNebat ToffikJamesNo ratings yet
- Ibn Sina FinalDocument10 pagesIbn Sina FinalHimelarifNo ratings yet
- Final A Research On State of Health in Comparison With HospitalDocument127 pagesFinal A Research On State of Health in Comparison With HospitalShivam JoshiNo ratings yet
- Pedoman Rawat InapDocument29 pagesPedoman Rawat InapNur AsriatiNo ratings yet
- DPHO Final EditedDocument24 pagesDPHO Final EditedBinita ShakyaNo ratings yet
- SMH Annual Report 2017Document7 pagesSMH Annual Report 2017Chelsey BoyleNo ratings yet
- Genral Nursing Midwiferyl Nursing Syllabus PDFDocument93 pagesGenral Nursing Midwiferyl Nursing Syllabus PDFRavindra Puranik Msc Nursing0% (1)
- Suci Sunarti P07524118163Document55 pagesSuci Sunarti P07524118163Dwi Woro WidayatiNo ratings yet
- An Organizational Analysis Presented To The College of NursingDocument8 pagesAn Organizational Analysis Presented To The College of NursingAnni BarbaNo ratings yet
- 1 Paper EmergencyDepartmentPatientProcessFlowDocument6 pages1 Paper EmergencyDepartmentPatientProcessFlowandika fahruroziNo ratings yet
- 1 Paper EmergencyDepartmentPatientProcessFlowDocument6 pages1 Paper EmergencyDepartmentPatientProcessFlowYey PahmateeNo ratings yet
- UPMC Children's Hospital of Pittsburgh Process Improvement Proposal.Document14 pagesUPMC Children's Hospital of Pittsburgh Process Improvement Proposal.lindsey02grayNo ratings yet
- Organizing NSG ServiceDocument28 pagesOrganizing NSG ServiceAnusha VergheseNo ratings yet
- Conference Book International Conference On Health Care and ManagementDocument18 pagesConference Book International Conference On Health Care and ManagementLinlin LindayaniNo ratings yet
- 39 77 1 SMDocument15 pages39 77 1 SMMata MataNo ratings yet
- Conference Book International Conference On Health Care and ManagementDocument15 pagesConference Book International Conference On Health Care and ManagementTaqiyuddin Akhmad Al-hakimNo ratings yet
- REV Report Management Group 1 Period 2-1Document26 pagesREV Report Management Group 1 Period 2-1anggi windiNo ratings yet
- Job Description - Specialty Doctor in General SurgeryDocument15 pagesJob Description - Specialty Doctor in General Surgeryvlad9100% (1)
- Nurse Practitioner. (Final)Document14 pagesNurse Practitioner. (Final)SamNo ratings yet
- Dup (1) PSM PROFILEDocument14 pagesDup (1) PSM PROFILEBobby BhatiyaNo ratings yet
- Motivational Factors of Nurses in A Group of Primary Health Centres in The City of Lisbon: Qualitative StudyDocument3 pagesMotivational Factors of Nurses in A Group of Primary Health Centres in The City of Lisbon: Qualitative StudyNur MiladiyahNo ratings yet
- To Become The World's Best Tertiary Healthcare ProviderDocument13 pagesTo Become The World's Best Tertiary Healthcare ProviderShah BrijeshkumarNo ratings yet
- Swot Analysis in Establishment of Nursing Service Quality in RS. TK. III DR Reksodiwiryo PadangDocument6 pagesSwot Analysis in Establishment of Nursing Service Quality in RS. TK. III DR Reksodiwiryo PadangInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- MAX Employment Retention Based On Employment SatisfactionDocument104 pagesMAX Employment Retention Based On Employment SatisfactionMahnaz AnsariNo ratings yet
- Critical Evaluation of Nursing Programme 2Document31 pagesCritical Evaluation of Nursing Programme 2Pearlson JebamarshelNo ratings yet
- A Clinical Report On Field Attachment at Matungu Sub - County HospitalDocument46 pagesA Clinical Report On Field Attachment at Matungu Sub - County HospitalJustin 037No ratings yet
- Importance of Support ServicesDocument5 pagesImportance of Support ServicesRockson Ohene AsanteNo ratings yet
- Assignment ON Continuing EducationDocument6 pagesAssignment ON Continuing EducationDebashrita MisraNo ratings yet
- English Project AnushDocument9 pagesEnglish Project AnushAashish SapkotaNo ratings yet
- Week 9 AssignmentDocument10 pagesWeek 9 Assignmentlindsey02grayNo ratings yet
- Symbiosis Institute of Health Sciences (Sihs)Document23 pagesSymbiosis Institute of Health Sciences (Sihs)Anshuman KhaitanNo ratings yet
- s12909 019 1740 6Document13 pagess12909 019 1740 6Hàn Nguyệt CátNo ratings yet
- Summer Training ReportDocument71 pagesSummer Training Reportshrutigoel23No ratings yet
- Final Proposal SubmissionDocument24 pagesFinal Proposal Submissionapi-551359614No ratings yet
- Evaluation of Nursing Programme On The Basis of MRPDocument12 pagesEvaluation of Nursing Programme On The Basis of MRPPRITI SHARMANo ratings yet
- DonnaEldridge PosterDocument1 pageDonnaEldridge PosterNHS Leadership AcademyNo ratings yet
- Organizing Nursing Services and Patient Care IntroductionDocument22 pagesOrganizing Nursing Services and Patient Care Introductionthanuja mathew83% (6)
- Patient Satisfaction Regarding Healthcare ServicesDocument30 pagesPatient Satisfaction Regarding Healthcare ServicesSagar Tanna67% (3)
- Manpowerplanning 140324112957 Phpapp01Document60 pagesManpowerplanning 140324112957 Phpapp01sagarbhingareNo ratings yet
- Importance and Purposes of Research: Instruction: Answer Comprehensively and ExtensivelyDocument3 pagesImportance and Purposes of Research: Instruction: Answer Comprehensively and ExtensivelyKarl Kiw-isNo ratings yet
- Supportive SupervisionPlan - September 2011Document19 pagesSupportive SupervisionPlan - September 2011Jay PaulNo ratings yet
- KDC Report 1juneDocument19 pagesKDC Report 1juneHarshada BhaleraoNo ratings yet
- Deblina Dutta Project A Study On Management of Ipd at RN Tagore Hospital 2 1 1Document55 pagesDeblina Dutta Project A Study On Management of Ipd at RN Tagore Hospital 2 1 1DAD SHOTSNo ratings yet
- LP Katim SHDocument31 pagesLP Katim SHiqbal rizky anandaNo ratings yet
- CASE REPORT - Addressing Nurse ShortageDocument27 pagesCASE REPORT - Addressing Nurse ShortageArchie Beringuel JavierNo ratings yet
- Five Year Hospital Strategic Plan ExampleDocument60 pagesFive Year Hospital Strategic Plan ExampleEsteban R. LangloisNo ratings yet
- Bioethics Assignment-7 - Public Health EthicsDocument1 pageBioethics Assignment-7 - Public Health EthicsIC BNo ratings yet
- Canterbury Strategic PlanDocument52 pagesCanterbury Strategic PlanMuhammad Agung BhagaskoroNo ratings yet
- Bab II Bag 1 FixDocument10 pagesBab II Bag 1 FixJimJim JimJimNo ratings yet
- Chapter 11Document4 pagesChapter 11Ramsel Kong Tan100% (1)
- (Tfih Fi M Ffi M - Il FfiDocument1 page(Tfih Fi M Ffi M - Il Ffione twoNo ratings yet
- Ecfmg: Information BookletDocument50 pagesEcfmg: Information Bookletone twoNo ratings yet
- 6-Month Usmle Step 1 Sample Schedule Day Event Subjects Pathoma TasksDocument15 pages6-Month Usmle Step 1 Sample Schedule Day Event Subjects Pathoma Tasksone twoNo ratings yet
- Form 900Document1 pageForm 900one twoNo ratings yet
- 6-Month Usmle Step 1 Sample ScheduleDocument14 pages6-Month Usmle Step 1 Sample ScheduleKhadijah Al HadiNo ratings yet
- Self Doc AttestDocument1 pageSelf Doc Attestone twoNo ratings yet
- Fees For Consular Services RevisedDocument1 pageFees For Consular Services Revisedone twoNo ratings yet
- PGDHCM RetakeDocument1 pagePGDHCM Retakeone twoNo ratings yet
- .:ftyafrsqm Rqidq, T Ffiq ,"R.: (@N. (O9Blobz,)Document4 pages.:ftyafrsqm Rqidq, T Ffiq ,"R.: (@N. (O9Blobz,)one twoNo ratings yet
- Manish Khanal Mobile: 9841842618Document1 pageManish Khanal Mobile: 9841842618one twoNo ratings yet
- वडा कार्यलयको प्रस्तावित कार्यविधि २०७०Document72 pagesवडा कार्यलयको प्रस्तावित कार्यविधि २०७०bharati adhikariNo ratings yet
- Cover Letter Sujan TamangDocument1 pageCover Letter Sujan Tamangone twoNo ratings yet
- Curriculum Vitae: Sagar KhadkaDocument2 pagesCurriculum Vitae: Sagar Khadkaone twoNo ratings yet
- Bidwata Rai Khumltar, Lalitpur, Nepal Contact No.: 9869075699 EmailDocument2 pagesBidwata Rai Khumltar, Lalitpur, Nepal Contact No.: 9869075699 Emailone twoNo ratings yet
- Sujan Lal TamangDocument5 pagesSujan Lal Tamangone twoNo ratings yet
- Sarmila CVDocument1 pageSarmila CVone twoNo ratings yet
- Proposal AnupaDocument31 pagesProposal Anupaone twoNo ratings yet
- Case StudyDocument44 pagesCase Studyone twoNo ratings yet
- TOR For Building DesignDocument2 pagesTOR For Building Designone twoNo ratings yet
- Soyan Shah CVDocument2 pagesSoyan Shah CVone twoNo ratings yet
- Curriculum Vitae of Ms. Pushpa SharmaDocument4 pagesCurriculum Vitae of Ms. Pushpa Sharmaone twoNo ratings yet
- Tender 30 075 076 Maintenance Items BOQDocument10 pagesTender 30 075 076 Maintenance Items BOQone twoNo ratings yet
- Yeti Health Science Acedamy ToolsDocument4 pagesYeti Health Science Acedamy Toolsone twoNo ratings yet
- Accounting Policies and Notes To The Accounts ofDocument1 pageAccounting Policies and Notes To The Accounts ofone twoNo ratings yet
- Ninhc Bank Account DetailsDocument1 pageNinhc Bank Account Detailsone twoNo ratings yet
- Staff QualificationvvvvvDocument12 pagesStaff Qualificationvvvvvone twoNo ratings yet
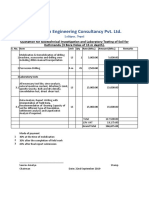
- Quotation For Soil TestDocument1 pageQuotation For Soil Testone twoNo ratings yet
- National Institute of Neurological and Heart Center Pvt. Ltd. Kathmandu, NepalDocument7 pagesNational Institute of Neurological and Heart Center Pvt. Ltd. Kathmandu, Nepalone twoNo ratings yet
- PKC and AssociatesDocument4 pagesPKC and Associatesone twoNo ratings yet
- 2023 Instructions For Suppliers - Delivery To Venray Singapore Ver1.25 - June2023Document14 pages2023 Instructions For Suppliers - Delivery To Venray Singapore Ver1.25 - June2023ceciliaNo ratings yet
- BPCS Shop OrderDocument69 pagesBPCS Shop OrderSushil Bhosale100% (1)
- Best Practice ViacombiDocument106 pagesBest Practice ViacombiFakoAmmarNo ratings yet
- Supply Chain Management: Dr. Ferdous SarwarDocument40 pagesSupply Chain Management: Dr. Ferdous SarwarAshad ChowdhuryNo ratings yet
- Importance of Management in Aviation: Dennis Kira, Golnaz Rezai, Raafat George SaadéDocument17 pagesImportance of Management in Aviation: Dennis Kira, Golnaz Rezai, Raafat George SaadéManel LanemNo ratings yet
- Spatialities of GlobalisationDocument16 pagesSpatialities of Globalisationjohnfcg1980No ratings yet
- Pacejet ROI Spreadsheet Shipping SoftwareDocument5 pagesPacejet ROI Spreadsheet Shipping SoftwareOmaid TariqNo ratings yet
- Courier ListDocument24 pagesCourier ListMonirHR0% (1)
- Vishal Mega Mart 1 PDFDocument58 pagesVishal Mega Mart 1 PDFbagal07No ratings yet
- Marine Insurance - LossesDocument20 pagesMarine Insurance - LossesShivam Kumar100% (1)
- Week 8 - Lecture - Vertical Integration 2021-S1Document32 pagesWeek 8 - Lecture - Vertical Integration 2021-S1Sam ChawlaNo ratings yet
- The Effect of Supply Chain Management Processes On Competitive Advantage and Organizational PerformanceDocument105 pagesThe Effect of Supply Chain Management Processes On Competitive Advantage and Organizational PerformanceAnwar AnwarNo ratings yet
- Warehouse Management System: Oracle WMSDocument30 pagesWarehouse Management System: Oracle WMSmuralikb234No ratings yet
- Parle G Sales and DistributionDocument34 pagesParle G Sales and DistributionShresth KotishNo ratings yet
- LSCM BrochureDocument7 pagesLSCM Brochurekgv_mailsNo ratings yet
- Integrated Logistic SupportDocument34 pagesIntegrated Logistic SupportZamri ZainalNo ratings yet
- SLM Lean Strategies.Document9 pagesSLM Lean Strategies.Raja Atiq Qadir SattiNo ratings yet
- Peachtree Networks IntroDocument11 pagesPeachtree Networks IntroMBilalA06No ratings yet
- Nbnfi Fe2020120799638Document7 pagesNbnfi Fe2020120799638Jerome PolicarpioNo ratings yet
- Transport Documents Used in International Trade PDFDocument5 pagesTransport Documents Used in International Trade PDFsatyaseerNo ratings yet
- Jnu Supply Chain ManagementDocument89 pagesJnu Supply Chain ManagementamaldhasapolloNo ratings yet
- 4903-Woodgrain Millwork Builds Their Success With SAP Transportation Management TM 9.0Document22 pages4903-Woodgrain Millwork Builds Their Success With SAP Transportation Management TM 9.0Prajal MeshramNo ratings yet
- St. Louis Regional Economic Adjustment Strategic Plan 2011 - AECOMDocument242 pagesSt. Louis Regional Economic Adjustment Strategic Plan 2011 - AECOMnextSTL.comNo ratings yet
- Franklin Attachment ReportDocument26 pagesFranklin Attachment ReportMiriam NaliakaNo ratings yet
- Understanding Zara's Supply ChainDocument7 pagesUnderstanding Zara's Supply ChainDYPUSM WECNo ratings yet
- Calculations On Loading & HaulageDocument24 pagesCalculations On Loading & HaulageSarah Mae Ajon95% (22)
- QB Logistics ManagementDocument10 pagesQB Logistics ManagementDivyaNo ratings yet
- Multi Modal Logistics HubDocument33 pagesMulti Modal Logistics HubsinghranjanNo ratings yet
- Ics Reading List 2016 WebDocument24 pagesIcs Reading List 2016 WebChristos AdNo ratings yet
- PESTEL AnalysisDocument8 pagesPESTEL AnalysisGokul Karwa33% (3)