You might also like
- 85 ADATranstornosAlimentaresDocument10 pages85 ADATranstornosAlimentaresJoana TavaresNo ratings yet
- Geron - Group 1Document11 pagesGeron - Group 1Potato TomatoNo ratings yet
- Treatment of Eating DisordersDocument4 pagesTreatment of Eating DisordersDave MondoyoNo ratings yet
- Aus Anorexia Nervosa PDFDocument31 pagesAus Anorexia Nervosa PDFYondri Mandaku Tasidjawa100% (1)
- Republic of The Philippines Tamag, Vigan City 2700 Ilocos SurDocument8 pagesRepublic of The Philippines Tamag, Vigan City 2700 Ilocos SurJewel Ramos GalinatoNo ratings yet
- Case StudyDocument3 pagesCase StudyAngelica Joyce SinnacoNo ratings yet
- B A P F I O: Ehavioral ND Sychological Actors N BesityDocument4 pagesB A P F I O: Ehavioral ND Sychological Actors N BesityUjian LancarNo ratings yet
- Eating DisorderDocument11 pagesEating Disorderapi-495417520No ratings yet
- The Ultimate Metabolism Diet: Eat Right for Your Metabolic TypeFrom EverandThe Ultimate Metabolism Diet: Eat Right for Your Metabolic TypeRating: 3 out of 5 stars3/5 (3)
- From Within: Exploring the Intricate Bond between Body Dysmorphic Disorder and Eating DisordersFrom EverandFrom Within: Exploring the Intricate Bond between Body Dysmorphic Disorder and Eating DisordersNo ratings yet
- Asesmen GeriatriDocument90 pagesAsesmen GeriatriTri Anggun UtamiNo ratings yet
- Problem and Its Background An Eating Problem Is Any Relationship With Food That Find DifficultDocument15 pagesProblem and Its Background An Eating Problem Is Any Relationship With Food That Find DifficultRose Ann ManaloNo ratings yet
- 234 FullDocument7 pages234 FullKim YusonNo ratings yet
- GeriDocument6 pagesGeriSetia BudiNo ratings yet
- Libro TCA - ANDDocument228 pagesLibro TCA - ANDCarpetas PSicologiaNo ratings yet
- Eating Disorder: What Are The Major Kinds of Eating Disorders?Document3 pagesEating Disorder: What Are The Major Kinds of Eating Disorders?Sunny KumarNo ratings yet
- Teaching Diabetes ManagementDocument5 pagesTeaching Diabetes ManagementWebster Claveria100% (5)
- Session #14 SAS - Nutrition (Lecture)Document7 pagesSession #14 SAS - Nutrition (Lecture)cabo.bontilao.swuNo ratings yet
- (Psychology) Eating Disorders - Psychotherapy's Role in Effective TreatmentDocument3 pages(Psychology) Eating Disorders - Psychotherapy's Role in Effective TreatmentolinaivanNo ratings yet
- FINAL Food Addiction Tool Kit 10-14-15Document59 pagesFINAL Food Addiction Tool Kit 10-14-15Torc Steele100% (1)
- Binge Eating DisorderDocument4 pagesBinge Eating Disordereneg4530100% (1)
- Binge Eating Disorder PDFDocument4 pagesBinge Eating Disorder PDFIsidora KesićNo ratings yet
- The Impact of Orem's Self-Care Model On The Quality of Life in Patients With Type II DiabetesDocument1 pageThe Impact of Orem's Self-Care Model On The Quality of Life in Patients With Type II DiabetesChristelle Marie De GuzmanNo ratings yet
- Coping strategies for managing ADHD symptomsDocument3 pagesCoping strategies for managing ADHD symptomsDaniel N OmuseNo ratings yet
- A Guide To Selecting Evidence-Based Psychological TherapiesDocument19 pagesA Guide To Selecting Evidence-Based Psychological Therapiesangela cabrejosNo ratings yet
- Cap 1Document11 pagesCap 1SofiaNo ratings yet
- Nutri Midterm NotesDocument52 pagesNutri Midterm NotesiyahNo ratings yet
- Aaa 2019 Nyt MmaDocument93 pagesAaa 2019 Nyt MmathanzeroNo ratings yet
- Geriatric Nursing Care Plan for Failure to ThriveDocument15 pagesGeriatric Nursing Care Plan for Failure to ThriveYongNo ratings yet
- Understanding Addiction: Causes, Treatments and Vulnerable GroupsDocument4 pagesUnderstanding Addiction: Causes, Treatments and Vulnerable GroupsIvin KuriakoseNo ratings yet
- NUTRITION AND DIET: EXERCISE, FOOD, AND NURSING CAREDocument2 pagesNUTRITION AND DIET: EXERCISE, FOOD, AND NURSING CAREPALEN, DONNA GRACE B.No ratings yet
- Question 1a Write Notes On Eating DisorderDocument19 pagesQuestion 1a Write Notes On Eating DisordermwakibiliNo ratings yet
- Behavioral Modification for Weight ManagementDocument17 pagesBehavioral Modification for Weight ManagementLudmila AraújoNo ratings yet
- Ethics of Artificial NutritionDocument3 pagesEthics of Artificial NutritionsobanNo ratings yet
- BSN-3A Geria Lab Week 1 - BOLDIOSDocument4 pagesBSN-3A Geria Lab Week 1 - BOLDIOSPsyche Valerie BoldiosNo ratings yet
- 5.ADA-Facilitating Behavior Change and Well-Being To Improve Health OutcomesDocument4 pages5.ADA-Facilitating Behavior Change and Well-Being To Improve Health OutcomesGianinaMihalacheCojocaruNo ratings yet
- Food Addiction Denial: False Information and Irrational ThinkingFrom EverandFood Addiction Denial: False Information and Irrational ThinkingNo ratings yet
- Chapter 014Document19 pagesChapter 014dtheart2821No ratings yet
- Psychological Impact of DiabetesDocument2 pagesPsychological Impact of DiabetesNeph BotorNo ratings yet
- Differnt Kinds of Eating DisordersDocument5 pagesDiffernt Kinds of Eating Disordersapi-610702943No ratings yet
- Eugenio, Aldwin Eugene. Empowering The Nation Against Diabetes. Diabetes Direction2007 Vol.1 No.3 pp.3-4Document7 pagesEugenio, Aldwin Eugene. Empowering The Nation Against Diabetes. Diabetes Direction2007 Vol.1 No.3 pp.3-4loulen2421No ratings yet
- Lit Review - Eating DisorderDocument4 pagesLit Review - Eating DisorderAlien4mearthNo ratings yet
- Dietary Management in Disease - IDocument28 pagesDietary Management in Disease - IPriya SoniNo ratings yet
- Nutrition's Role in Addiction RecoveryDocument50 pagesNutrition's Role in Addiction Recoverystacia666100% (2)
- Gonzales NutriDocument2 pagesGonzales Nutri17melrosefloresNo ratings yet
- Nutrition in Addiction RecoveryDocument50 pagesNutrition in Addiction Recoverylillith1723100% (1)
- Case 1Document25 pagesCase 1hamshiniNo ratings yet
- Fall Prevention: How Can Older Adults Prevent Falls?Document4 pagesFall Prevention: How Can Older Adults Prevent Falls?Amalina ZahariNo ratings yet
- Eating DisorderDocument26 pagesEating Disordernoot_onNo ratings yet
- Diabetes Disease ManagementDocument7 pagesDiabetes Disease ManagementNashNo ratings yet
- Scenario One Diabetes (Sweet A 2018-1Document5 pagesScenario One Diabetes (Sweet A 2018-1Regina PunNo ratings yet
- Change Behavior To Adopt A Healthier Lifestyle.: AlcoholDocument20 pagesChange Behavior To Adopt A Healthier Lifestyle.: AlcoholAlberto NorrisNo ratings yet
- Vera Geanella Critical Care Assignment FinalDocument8 pagesVera Geanella Critical Care Assignment Finalapi-496082089No ratings yet
- Vera Geanella Food Allergies and IntolerancesDocument1 pageVera Geanella Food Allergies and Intolerancesapi-496082089No ratings yet
- AllaroundpennsaukenDocument1 pageAllaroundpennsaukenapi-496082089No ratings yet
- Prebiotics FinalDocument1 pagePrebiotics Finalapi-496082089No ratings yet
- Ef Lab ProjectDocument18 pagesEf Lab Projectapi-496082089No ratings yet
- Experiment Foods Lab ReportDocument15 pagesExperiment Foods Lab Reportapi-496082089No ratings yet
- Lesson Plan Final NFDocument7 pagesLesson Plan Final NFapi-496082089No ratings yet
- Community Assessment - Teen Girls Pa - FinalDocument29 pagesCommunity Assessment - Teen Girls Pa - Finalapi-496082089No ratings yet
- Patient Summary Extra CreditDocument1 pagePatient Summary Extra Creditapi-496082089No ratings yet
- BloominginspringupdatedDocument1 pageBloominginspringupdatedapi-496082089No ratings yet
- Nursing and Midwifery Board Candidate Handbook RN OSCE ExaminationDocument25 pagesNursing and Midwifery Board Candidate Handbook RN OSCE ExaminationkemalayazNo ratings yet
- EGZOTech Luna EMG Brochure 2018 With LogoDocument13 pagesEGZOTech Luna EMG Brochure 2018 With LogoApostolis KopoukisNo ratings yet
- 9 Types of Female Orgasms ExplainedDocument4 pages9 Types of Female Orgasms ExplainedAbdul SyukurNo ratings yet
- Umftgm 2017 MarissiensisDocument148 pagesUmftgm 2017 MarissiensisAdriana VillarrealNo ratings yet
- Grand Unification For World Peace Music THerapy For Integrating Healthcare PDFDocument339 pagesGrand Unification For World Peace Music THerapy For Integrating Healthcare PDFDr Suvarna NalapatNo ratings yet
- Chapt01 The Sudy of ChangeDocument34 pagesChapt01 The Sudy of ChangeIkhsan Abdul HanifNo ratings yet
- Fat-Burning FoodsDocument11 pagesFat-Burning FoodsRamzi FaddoulNo ratings yet
- Causes of Baby Dumping: Family Breakups, Lack of Education, and PovertyDocument2 pagesCauses of Baby Dumping: Family Breakups, Lack of Education, and Povertysirthana697547No ratings yet
- Reading Skills in 350 WordsDocument16 pagesReading Skills in 350 WordsCarthy Tang100% (2)
- Trays PDFDocument18 pagesTrays PDFBilal Hasan100% (1)
- Hypertension Scope and Limitations HomoeopathyDocument4 pagesHypertension Scope and Limitations HomoeopathyZubs .....No ratings yet
- Maynilad Valenzuela Sewerage Project Environmental ReportDocument297 pagesMaynilad Valenzuela Sewerage Project Environmental ReportmarvilouNo ratings yet
- Neem by Ellen NortenDocument100 pagesNeem by Ellen NortenMano DrabuzeliaiNo ratings yet
- 4.schedule Waste Management UTM - SWMP - 22mei2018 PDFDocument54 pages4.schedule Waste Management UTM - SWMP - 22mei2018 PDFfaraNo ratings yet
- Low Endotoxin Recovery (LER) in Drug Products - Original - 31428Document2 pagesLow Endotoxin Recovery (LER) in Drug Products - Original - 31428Putri DozanNo ratings yet
- Intern Performance Review TemplateDocument3 pagesIntern Performance Review TemplatePrincess Joan InguitoNo ratings yet
- Evaluation and Treatment of Aphasia Among The Elderly With StrokeDocument11 pagesEvaluation and Treatment of Aphasia Among The Elderly With StrokemgpastorNo ratings yet
- Artificial InseminationDocument3 pagesArtificial Inseminationapi-263932656No ratings yet
- SSIPDocument4 pagesSSIPGlenn Clemente100% (2)
- Prevalence of GERD in Dyspepsia PatientsDocument6 pagesPrevalence of GERD in Dyspepsia PatientsAbrar TaraNo ratings yet
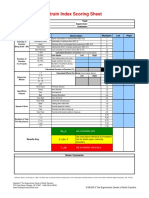
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- Global Urology Devices MarketDocument14 pagesGlobal Urology Devices MarketNamrataNo ratings yet
- Synthesis 3 Jay VillasotoDocument6 pagesSynthesis 3 Jay VillasotoJay VillasotoNo ratings yet
- Guided Reflection 2Document4 pagesGuided Reflection 2Summer SeedsNo ratings yet
- 4) Skema Set 1Document10 pages4) Skema Set 1Raymond Cheang Chee-CheongNo ratings yet
- Appendix7 I-131Document4 pagesAppendix7 I-131Crizzz001No ratings yet
- Concussionspaper 1Document6 pagesConcussionspaper 1api-350027909No ratings yet
- 8 RA 4688 (Clinical Laboratory Law)Document32 pages8 RA 4688 (Clinical Laboratory Law)AIRRA CLAIRE ALVAREZNo ratings yet
- Grief & Grieving ProcessDocument39 pagesGrief & Grieving Processelmerconde100% (4)
- Can Mindfulness in Health Care Professionals Improve Patient Care An Integrative Review and Proposed Model.Document15 pagesCan Mindfulness in Health Care Professionals Improve Patient Care An Integrative Review and Proposed Model.ALIXNo ratings yet