PERIOPERATIVE ERAC PATHWAY ELEMENTS
9 Elements,
5 Elements
ERAC
ice arco olA)
ciety for Obstetric Anestl
Consensus Statement and
Enhanced Recovery A\
LIMIT FASTING
INTERVAL
Comments
‘Reduces aspiration risk while limiting hypovoe-
mia, metabolic stress, and ketosis.
+ Data extrapolated from colorectal ERAS
Solids up to 8h
before cesarean
delivery
programs
ASA guidelines state 6-8 hhased on We type
of ood ingested:
+ Alignt meal or mk may be ingested for up
to 6h before elective procedures requiring
{eneral anesthesia regional anesthesia, oF
‘procedural sedation and analgesic
+ Additional fasting ime (8 or more hours) may
be needed in cases of patent intake of ed
foods, faty foods, oF meat
Nonparticulate
liq carbo loading
( TY Nonparticulate carbohydrate drink up to 2 h before
i _ cesarean delivery (nondiabetic women only)
oo™
D 45 g carbohydrate is recommended
\
f ») Examples: Gatorade 32 oz (54 g carbohydrate) clear
\,__/ apple juice 16 02 (56 & carbohyérate)
>
+ Reduces matemel hypogycemia and
‘metabolic stress
+ The beneit of complex cabohydate (eg,
‘maltodexri) cinks for cesarean delivery is
‘currently undefined, and fetal effects unknown
+ Can omit if mother is diabetic; follow
Institutional protocols for matemal diabetes/
monitoring
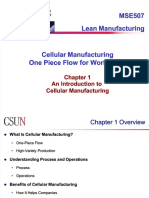
STANDAR RESEP MINUMAN TINGGI KARBOHIDRAT PRE OPERASI TEKNIK ERACS
400 ML : 335 KALORI (1 CC: 0,8 ML)
.NDUNGAN GIZI
NO|| NAMABANAN BERAT _[ ENERGI(KKAL) | PROTEIN) | LEMAK (@) | KANG)
1_|AIR PUTIN. 400 ML o 0 oO 0
2 _|MALTODEKSTRIN _|30 GRAM 144 0 0 45,6
3_|GULA PASIR 130 GRAM. us oO 0 ZUF-
4 |JERUK MANIS 150 GRAM. 75 i) 0 18
S_|GARAM. ISECUKUPNYA_ oO oO 0 0
TOTAL 334 o fe 91,3
Patient
Education
= >> Ideal: Direct contact with patients with phone
| call/reminder or meeting before cesarean, to remind
ae _/ patient of ERAC goals
zo
/oN
( \ Minimum: Handout or other standardized
\__/ educational to! or interaction
( ) Example: SOAP videos available on www. SOAP.org
+The goal of ERAC patient education isto set
‘expectations, and to engage/empower the
patent to participate more completely in thee
‘care plan and recovery
+ Ideally, patient education takes place before
‘the day of surgery
+ Preoperative discussion should include ERAC
gos in addon tothe routine preeratve
Lactation/breastfee
ding preparation &
education
Ideal: Structured prenatal classes with books,
videos, and in-person lactation support in the
/ hospital
Minimum: Handout or other standardized tool or
interaction that includes information on normal
breastfeeding physiology, management of
/ common lactation complications, and resources
for breastfeeding support after discharge
+ ay brestledig improves nexbom and
rraeal utes nd pat
emovonal attachment, reduced intent
inet colons, deed kr
‘sudden infant death syndrome
+ Breastfeeding is pubic heath pity
because tis ik protect foo”
dese heath acne such
INTRAOPERATIVE ERAC PATHWAY 11 ELEMEN
eM han recast
+ Spinal anesthesia-associated hypoten-
‘lon is primanily on afteroaddriven
Goal Isto prevent intraoperative
ae posi
Maintain blood ves
pressure at ‘anesthesia and maintain
baseline uteroplacental perfusion
+ Vasopressor regimen may need to be
modifies in women with preeclampsia
Optimally managed with prophylactic ‘28 the degree of hypotension with
vasopressor infusion, for example, ‘spinal anesthesia may be less than
phenylephrine (or norepinephrine) infusion ‘that in nonpreeciamptics-
+ Data are well supported in terature
INTRAOPERATIVE ERAC PATHWAY ELEMENTS
oa aaa
+ Corie ace warming ating
rena
SSM cure
INTRAOPERATIVE ERAC PATHWAY ELEMENTS
ee MU re cl
Pere
+ Inthe case of bemonhage caused by
‘erin ator. transition from ERAC to
eae cane eeu acca Insttons| nemormage resuscitation
Prete enc une s ue ea Mac) ‘protocol
Bolus 1 1U oxytocin; start oxytocin infusion at
"2.57.5 IU-h* (0.04-0.125 1U-min!)
-and intrapartum cesarean delivery:
31U oxytocin over =30 : start oxytocin
infusion at 7.5-15 IU: * (0.125-0.25
twin?
INTRAOPERATIVE ERAC PATHWAY ELEMENTS
INTRAOPERATIVE ERAC PATHWAY ELEMENTS
ene
EU I
Weasel
= Skin-to-skin contact should occur as soon as possible in the operating room as
appropriate based on maternal/neonatal condition
is
j lee area Ye]
eyez cola)
Limit intravenous fluids to < 3L for routine cases
In the case of hemorrhage, transition from ERAC to institutional hemorrhage
ote cass)
SM ee oa aca UC nS
primarily managed with vasopressors, instead of fluids
eee ory oe Sere
established
INTRAOPERATIVE ERAC PATHWAY ELEMENTS
Delayed Umbilical
Cord clamping
Benefts: Ter: improved iron stores, develorental benefits;
‘ete: iproved tanstona relation reduced ree for
am nm
‘vrei henoxtage
+ Does rot nerease matemal risk for bood loss or transfusion
~The pride dye craig may vay aang
Inston and settings
Dele cud dang stl be oe a cert stuns,
tera nally, eeatl ned fo nmediate esusctation)*
OF POSTOPERATIVE ERAC PATHWAY ELEMENTS
Ice chips and/or water within 60 min
| ies Ext or ita est:
postcesarean admission to PACU sydney
+ Reduced hospital gh of tay
Heparin/saline lock the IV early once ist spec peepee
oxytocin infusion complete, tolerating ————————— cuntig
fluids, and urine output adequate + Reduced postoperative catabolism
+ irved insulin sett
+ Reduced sical sess response
| ance to regular diet ideally within 4 h
cesarean, as tolerated
aA ea Ue a ela)
+ Ambulate only after adequate retum of
motor function | Early mobilization decreases:
Examples: Insulin resistance
0-8 h postoperatively: + Muscle atropty
= Siton edge of bed Hypoa
+ Out of bed to ehait + Venous thromboembolism
+ Ambulation a8 tolerated + Leng of stay
8-24 h postoperatively: Remove bamiers to early mobilization:
+ Ambulation as tolerated V poles
+ Walk: 1-2 times (or more) in hal + Urinary catheters
24-88 h postoperatively: + Poor pain contol
+ Wail: 3-4 times (or more) in hal + Sedation
+ Out of bed for & h se
+ Slow block regression
POSTOPERATIVE ERAC PATHWAY ELEMENTS
(2) Promotion of = Opin sep and rest + Fatigue potently enact ognitive hss Level CEO
resing prods Encounge clustered itenentions (eg, function depression, ain, mterrafant
tl sigs assessments incooinaton bonding, andrsk of respatary depression
‘wth anges ainsi: tring of
‘ra arlgesicsconteporaneoush
opopite seo postoperaie
tonto se SOAP eu
opine monitoring consensus
statemert®)
an
POSTOPERATIVE ERAC PATHWAY ELEMENTS
Benefits incu:
* Improved ambulation
+ Reduced length of stay
* Lower ates of symptomatic UT
ari catheter emoval may be asscited
ith higher rates of urinary retention and
‘eed for recateterization
Dose of neural tcl anesthetic and oid
‘an impact eateter removal tne
Urinary catheter removed by 6-12
h postpartum
Construct protocols to establish
criteria for appropriate removal and
to manage postcatheter removal
urinary retention
POSTOPERATIVE ERAC PATHWAY ELEMENTS
Follow instutional practices as per ACOG Cesarean delivery approximately doubles,
and ACCP guidelines! the ik of venous thromooembalsm
‘compare to vagal delve but in
otherwise heady patients the absolute Fisk
ielow
‘ACOG recommends mechanical
‘tromboembolsm proptans foal
‘women not already receiving pharmacoogle
‘tvemboprontyans™
aes
POSTOPERATIVE ERAC PATHWAY ELEMEN
(Oca exty — Sandricedscage paring ad» Dict plangon POD snd) Classe C0
Cischage sore cam str reopen pda ett, aed
+ Estland ralseaty crete ping
+ esol patent cree oid
oresibegat dstage
+ Use mest mano patent press
inmeatng ey tae cet
POSTOPERATIVE ERAC PATHWAY ELEMENTS
POSTOPERATIVE ERAC PATHWAY ELEMENTS
Multimodal analgesia protocols include:
+ Low-dose long-acting neuraxal opioid such as
‘morphine (see above)
+ Scheduled NSAID
+ Scheduled APAP
+ Local anesthetic techniques as indicated
Example:
+ APAP 650-1000 me Bral, per os ah scheduled
+ Ibuprofen 600 mg orally, per es qh scheduled
‘after IV ketorolac 45-30 mg was gven after
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Rekap Jam Induksi Elektif 11 Juni 2021Document6 pagesRekap Jam Induksi Elektif 11 Juni 2021DendyNo ratings yet
- Laporan Kasus - Dendy Dwi Ramadhani - PPDS Anestesi BrawijayaDocument1 pageLaporan Kasus - Dendy Dwi Ramadhani - PPDS Anestesi BrawijayaDendyNo ratings yet
- Adrenergic Agonist: Persiapan CBT September 2020 Bimo Kusumo BhirowoDocument16 pagesAdrenergic Agonist: Persiapan CBT September 2020 Bimo Kusumo BhirowoDendyNo ratings yet
- PDF Sosialisasi Eracs - CompressDocument22 pagesPDF Sosialisasi Eracs - CompressDendyNo ratings yet
- TEG® Analysis: Sample Data: Normal Values: CPT/Billing Codes: UnitsDocument1 pageTEG® Analysis: Sample Data: Normal Values: CPT/Billing Codes: UnitsDendyNo ratings yet
- Jadwal Jaga Chief Bulan Juni 2021 SMF Anestesiologi Dan Terapi IntensifDocument6 pagesJadwal Jaga Chief Bulan Juni 2021 SMF Anestesiologi Dan Terapi IntensifDendyNo ratings yet
- Rekap Ilmiah Ppds UpdateDocument63 pagesRekap Ilmiah Ppds UpdateDendyNo ratings yet
- Laporan Jaga P1: Minggu Malam, 28 Februari 2021Document16 pagesLaporan Jaga P1: Minggu Malam, 28 Februari 2021DendyNo ratings yet
- Relationship of D-Dimer With Severity and Mortality in Sars-Cov-2 Patients: A Meta-AnalysisDocument6 pagesRelationship of D-Dimer With Severity and Mortality in Sars-Cov-2 Patients: A Meta-AnalysisDendyNo ratings yet
- Data Undangan PPDS Hari Kamis Tgl. 04.02.2021 - MajapahitDocument15 pagesData Undangan PPDS Hari Kamis Tgl. 04.02.2021 - MajapahitDendyNo ratings yet
- Laporan Jaga Ok Igd: Selasa Malam, 9 Februari 2021Document4 pagesLaporan Jaga Ok Igd: Selasa Malam, 9 Februari 2021DendyNo ratings yet
- Physiologic Effects of Mechanical VentilatorDocument12 pagesPhysiologic Effects of Mechanical VentilatorDendyNo ratings yet
- Program Studi Anestesiologi Dan Terapi IntensifDocument2 pagesProgram Studi Anestesiologi Dan Terapi IntensifDendyNo ratings yet
- Staphylococcus Coagulase NegatifDocument8 pagesStaphylococcus Coagulase NegatifDendyNo ratings yet
- Dosis Obat CABG Ny SUNANIK 16 DES 2019Document1 pageDosis Obat CABG Ny SUNANIK 16 DES 2019DendyNo ratings yet
- SURAT KETERANGAN ResidentDocument1 pageSURAT KETERANGAN ResidentDendyNo ratings yet
- Morgan (Kumpulan Tabel)Document107 pagesMorgan (Kumpulan Tabel)Rian ArmiNo ratings yet
- Laporan Bulanan ICU RSSA November 2018Document13 pagesLaporan Bulanan ICU RSSA November 2018DendyNo ratings yet