You might also like
- Lec 35Document10 pagesLec 35محمد جاسم محمد عجاجNo ratings yet
- Lec: TMJ DR - Nawres BahaaDocument13 pagesLec: TMJ DR - Nawres BahaaMarwa AlfuaadiNo ratings yet
- Temporomandibular Joint and Muscles of Mastication: ContentsDocument38 pagesTemporomandibular Joint and Muscles of Mastication: ContentsDan 04No ratings yet
- Temporomandibular JointDocument15 pagesTemporomandibular Jointwasim hussainNo ratings yet
- Temporomandibular JointDocument86 pagesTemporomandibular Jointdrpankajaapaliya100% (2)
- Examinationoftmjmusclesofmastication2 140115105518 Phpapp02Document79 pagesExaminationoftmjmusclesofmastication2 140115105518 Phpapp02Dr. Anjana MaharjanNo ratings yet
- Mandibular MovementsDocument36 pagesMandibular MovementsRagini ShravanNo ratings yet
- TMJ AnatomyDocument68 pagesTMJ AnatomyArchanaShenoyNo ratings yet
- Tempero Mandibular JointDocument30 pagesTempero Mandibular JointAkash AmbhoreNo ratings yet
- Makalah ModulDocument55 pagesMakalah ModulVirena GunawanNo ratings yet
- Tempromanndibular JointDocument10 pagesTempromanndibular Jointehab radmanNo ratings yet
- Biomechanics of Temporomandibular Joint and Cervical SpineDocument60 pagesBiomechanics of Temporomandibular Joint and Cervical SpineRitika SonyNo ratings yet
- Anatomy and Bio Mechanics of The TMJDocument41 pagesAnatomy and Bio Mechanics of The TMJUmair KhanNo ratings yet
- TMJ and Muscles of MasticatoryDocument9 pagesTMJ and Muscles of MasticatoryFatima MartinezNo ratings yet
- Biomechanics of Temporomandibular JointDocument87 pagesBiomechanics of Temporomandibular JointseemaNo ratings yet
- 5 Relevant AnatomyDocument41 pages5 Relevant AnatomyKrupali JainNo ratings yet
- TMJ & Its MovementsDocument26 pagesTMJ & Its Movementsdeepinder27100% (1)
- TMJ Anatomy and Function GuideDocument100 pagesTMJ Anatomy and Function GuideMithileshwari Patil100% (1)
- TMJDocument40 pagesTMJARIF PUJI LAKSONONo ratings yet
- Functional Anatomy and TMJ PathologyDocument15 pagesFunctional Anatomy and TMJ PathologyJASPREETKAUR0410100% (1)
- Functional Anatomy of The Masticatory System, Part 1Document50 pagesFunctional Anatomy of The Masticatory System, Part 1اسراء اكرم هيمونيNo ratings yet
- The Temporomandibular Joint & Jaw BonesDocument8 pagesThe Temporomandibular Joint & Jaw Bonesبراءة أحمد السلاماتNo ratings yet
- The anatomy and development of the temporomandibular jointDocument13 pagesThe anatomy and development of the temporomandibular jointRajat NangiaNo ratings yet
- Anatomy of Temporomandibular Joint: Presented byDocument124 pagesAnatomy of Temporomandibular Joint: Presented bylkjhgfdsalkNo ratings yet
- TMJ Surgical Anatomy and ApproachesDocument165 pagesTMJ Surgical Anatomy and Approachesmohammad ghouseNo ratings yet
- Anatomy, Head and Neck, Temporomandibular Joint - StatPearls - NCBI BookshelfDocument8 pagesAnatomy, Head and Neck, Temporomandibular Joint - StatPearls - NCBI BookshelfDrishti ShahNo ratings yet
- Interchondral LigamentsDocument8 pagesInterchondral LigamentsAlina MoiseNo ratings yet
- TMJ AnatomiDocument53 pagesTMJ AnatomiNiTa DöéMy HarDianaNo ratings yet
- TMJ - Lec8Document10 pagesTMJ - Lec8A.A. HusseinNo ratings yet
- Section I #18 The Temporomandibular JointDocument3 pagesSection I #18 The Temporomandibular JointInnocent L NdambakuwaNo ratings yet
- TMJ Anatomy - OrthoDocument85 pagesTMJ Anatomy - Orthosamar yousif mohamedNo ratings yet
- TMJ WordDocument21 pagesTMJ WordBharathi GudapatiNo ratings yet
- Sama Notes Upper LimbDocument15 pagesSama Notes Upper LimbMaiUyen Kieu50% (2)
- TMJ CompleteDocument54 pagesTMJ CompleteNeal Torwane100% (3)
- Temporomandibular Joint: DR Bhaumik Thakkar MDS-Part 1. Dept. of Periodontology and ImplantologyDocument60 pagesTemporomandibular Joint: DR Bhaumik Thakkar MDS-Part 1. Dept. of Periodontology and ImplantologyJoseph Eduardo Villar CordovaNo ratings yet
- Anatomy and Physiology of Temporomandibular JointDocument16 pagesAnatomy and Physiology of Temporomandibular JointAsfoor gake1No ratings yet
- Temporomandibular Joint-127273Document9 pagesTemporomandibular Joint-127273raxNo ratings yet
- 5th Stage: - NazhatDocument11 pages5th Stage: - Nazhatعلي صادق جعفرNo ratings yet
- Temporo Mandibular JointDocument60 pagesTemporo Mandibular JointchaitreeNo ratings yet
- TMJ Surgical Anatomy GuideDocument11 pagesTMJ Surgical Anatomy GuideArchanaShenoyNo ratings yet
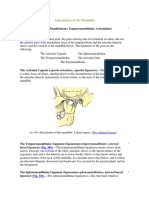
- The Articulation of The MandibleDocument4 pagesThe Articulation of The Mandibleviorel79No ratings yet
- Dental Histology Lecture on Temporomandibular JointDocument70 pagesDental Histology Lecture on Temporomandibular JointAMIT GUPTANo ratings yet
- TMJ Part 2Document31 pagesTMJ Part 2api-324160601No ratings yet
- 1.review OsteoarthritisDocument22 pages1.review OsteoarthritisGERSON RYANTONo ratings yet
- TMJOH محولDocument8 pagesTMJOH محولSafura IjazNo ratings yet
- Okeson 2007Document19 pagesOkeson 2007Duy ChâuNo ratings yet
- Lecture 7Document24 pagesLecture 7dr.sarahmajed23No ratings yet
- TMJ PrintDocument135 pagesTMJ PrintAsmaa RagabNo ratings yet
- TMJ Anatomy Study GuideDocument3 pagesTMJ Anatomy Study GuideSamer Tarek100% (1)
- Functional Anatomy of Temporomandibular JointDocument44 pagesFunctional Anatomy of Temporomandibular JointRomzi Hanif0% (1)
- JointsDocument27 pagesJointsVarsha Mol MohananNo ratings yet
- Joints: Dr. Vidhya Department of AnatomyDocument27 pagesJoints: Dr. Vidhya Department of Anatomyelan suriyanNo ratings yet
- Elbow and Antebrachium NotesDocument8 pagesElbow and Antebrachium NoteschadNo ratings yet
- Temporo: MandibularDocument38 pagesTemporo: MandibularyomanNo ratings yet
- Dr. JaffarDocument39 pagesDr. JaffarSyed Jaffar Abbas ZadiNo ratings yet
- Examen FisicoDocument26 pagesExamen FisicoAmada Angel VillanuevaNo ratings yet
- TMJ 2.0Document13 pagesTMJ 2.0Janvi RwtNo ratings yet
- Knee 05102018Document24 pagesKnee 05102018Dk KNo ratings yet
- TMJ PPT 130516130311 Phpapp02Document120 pagesTMJ PPT 130516130311 Phpapp02Hoang NhanNo ratings yet
- Sialography CTDocument4 pagesSialography CTNegin HekmatjooNo ratings yet
- Salivary GlandsDocument4 pagesSalivary GlandsNegin HekmatjooNo ratings yet
- Biomechanics of The (II)Document34 pagesBiomechanics of The (II)Negin HekmatjooNo ratings yet
- Sjogren Syndrome Xerostomia Traumatic ApaliDocument4 pagesSjogren Syndrome Xerostomia Traumatic ApaliNegin HekmatjooNo ratings yet
- Glossopharyngeal NeuralgiaDocument3 pagesGlossopharyngeal NeuralgiaNegin HekmatjooNo ratings yet
- Obstructive Salivary Gland Disease & Sialadenitis Causes, Symptoms, TreatmentDocument4 pagesObstructive Salivary Gland Disease & Sialadenitis Causes, Symptoms, TreatmentNegin HekmatjooNo ratings yet
- Neuropathic Pains Trigeminal NerveDocument6 pagesNeuropathic Pains Trigeminal NerveNegin HekmatjooNo ratings yet
- Obstructive Salivary Gland Disease & Sialadenitis Causes, Symptoms, TreatmentDocument4 pagesObstructive Salivary Gland Disease & Sialadenitis Causes, Symptoms, TreatmentNegin HekmatjooNo ratings yet
- Glossopharyngeal NeuralgiaDocument3 pagesGlossopharyngeal NeuralgiaNegin HekmatjooNo ratings yet
- Oral Tuberculosis: Negin Hekmatjoo (1702169) Armin Hekmatjoo (1702183)Document12 pagesOral Tuberculosis: Negin Hekmatjoo (1702169) Armin Hekmatjoo (1702183)Negin HekmatjooNo ratings yet
- Cardiovascular, Circulatory, and Hematologic FunctionDocument43 pagesCardiovascular, Circulatory, and Hematologic FunctionNegin HekmatjooNo ratings yet
- HypertentionDocument22 pagesHypertentionNegin HekmatjooNo ratings yet
- B9780702031458000788 WebDocument4 pagesB9780702031458000788 WebNegin HekmatjooNo ratings yet
- Biomechanics of The (II)Document34 pagesBiomechanics of The (II)Negin HekmatjooNo ratings yet
- Anatomy of The Temporomandibular JointDocument14 pagesAnatomy of The Temporomandibular JointRozi PiresNo ratings yet
- MUSCLES OF MASTICATION PRDocument3 pagesMUSCLES OF MASTICATION PRjohn mwambuNo ratings yet
- Temporalis Muscle Flap-1Document5 pagesTemporalis Muscle Flap-1Mohd Rehan QureshiNo ratings yet
- Space InfectionsDocument79 pagesSpace Infectionssridevi sivaramakrishnanNo ratings yet
- Cat Muscles 2Document3 pagesCat Muscles 2nathan3602No ratings yet
- Jns 1987 67 3 0463Document4 pagesJns 1987 67 3 0463mohNo ratings yet
- Comparative AnatomyDocument38 pagesComparative AnatomyKimm Charmaine RodriguezNo ratings yet
- The Muscles of Facial Expression (Skull 4)Document5 pagesThe Muscles of Facial Expression (Skull 4)زين العابدين محمد عويشNo ratings yet
- Tripod FractureDocument45 pagesTripod Fracturekenn ParrochoNo ratings yet
- Juvenile Nasopharyngeal Angiofibroma SurgeryDocument18 pagesJuvenile Nasopharyngeal Angiofibroma Surgeryarief ardaNo ratings yet
- RAdiology Related Infratemporal Fossa, Pterygo Palatine Fossa, Parapharyngeal SpaceDocument11 pagesRAdiology Related Infratemporal Fossa, Pterygo Palatine Fossa, Parapharyngeal SpacehaneefmdfNo ratings yet
- @ebookmedicin 2017 Clinical HeadDocument75 pages@ebookmedicin 2017 Clinical HeadDavid Esmeral Ojeda100% (1)
- Muscles of MasticationDocument27 pagesMuscles of MasticationNanditha Swaroop100% (2)
- Muscles of MasticationDocument6 pagesMuscles of MasticationAbdallah Essam Al-ZireeniNo ratings yet
- Oral Physio Slides - 5.mastication Dynamics of OcclusionDocument48 pagesOral Physio Slides - 5.mastication Dynamics of OcclusionMuhammadHafizZainudinNo ratings yet
- DC-TMD English Assessment Instruments - 2020 - 02 - 06 - SecuredDocument50 pagesDC-TMD English Assessment Instruments - 2020 - 02 - 06 - SecuredXiomara Reyes PalominoNo ratings yet
- Muscles of Mastication: DR Gauri MulayDocument57 pagesMuscles of Mastication: DR Gauri MulayAbhishek GuptaNo ratings yet
- Muscles of Mastication: Prof. Peter Stanko, MD, PHD Oral and Maxillofacial SurgeonDocument19 pagesMuscles of Mastication: Prof. Peter Stanko, MD, PHD Oral and Maxillofacial SurgeonVasantha RajanNo ratings yet
- A Revised Neuromyofascial Understanding For The Neck Head and Facial Channel Sinews Based On The Ling ShuDocument17 pagesA Revised Neuromyofascial Understanding For The Neck Head and Facial Channel Sinews Based On The Ling ShuAnonNo ratings yet
- Osteology of Maxilla & Mandible Muscles of MasticationDocument26 pagesOsteology of Maxilla & Mandible Muscles of MasticationJaveria KhanNo ratings yet
- Anatomy of Fat Pads CotofanaDocument15 pagesAnatomy of Fat Pads Cotofanadominique100% (2)
- Kaban 2009 TMJ ANKYLOSISDocument13 pagesKaban 2009 TMJ ANKYLOSISPorcupine TreeNo ratings yet
- Muscles of MasticationDocument106 pagesMuscles of MasticationShivam SharmaNo ratings yet
- Infratemporalna FossaDocument64 pagesInfratemporalna FossaJelena TasikNo ratings yet
- Dr Ahmed Fathalla Ibrahim's Guide to the Temporal and Infratemporal FossaeDocument11 pagesDr Ahmed Fathalla Ibrahim's Guide to the Temporal and Infratemporal FossaeMohammed EliasNo ratings yet
- Deep Neck Spaces PDFDocument15 pagesDeep Neck Spaces PDFSuprit SnNo ratings yet
- Muscle of Mastication and Its Role in Prosthodontics (Autosaved)Document42 pagesMuscle of Mastication and Its Role in Prosthodontics (Autosaved)Ramya Srinivasan67% (3)
- Muscles of Mastication Functions and Clinical SignificanceDocument130 pagesMuscles of Mastication Functions and Clinical SignificanceDevanand GuptaNo ratings yet
- Regional FlapsDocument55 pagesRegional Flapsswethakari100% (1)
- Surgical AnatomyDocument44 pagesSurgical AnatomyVishalKumarNo ratings yet
- Zygomatic FXDocument9 pagesZygomatic FXAmisha SilwalNo ratings yet