You might also like
- Judith Blaine (Eds.) - Proteinuria - Basic Mechanisms, Pathophysiology and Clinical Relevance-Springer International Publishing (2016)Document147 pagesJudith Blaine (Eds.) - Proteinuria - Basic Mechanisms, Pathophysiology and Clinical Relevance-Springer International Publishing (2016)Rubén Casas BenítezNo ratings yet
- Review of Linagliptin For The Treatment of Type 2 DiabetesDocument13 pagesReview of Linagliptin For The Treatment of Type 2 DiabetesMamad TrihatmowidjoyoNo ratings yet
- Exercise Improves Cardiovascular Control in A Model of DislipidemiaDocument5 pagesExercise Improves Cardiovascular Control in A Model of DislipidemiaMamad TrihatmowidjoyoNo ratings yet
- Impact of Metabolic Syndrome and Its Severity On Microvascular ComplicationsDocument5 pagesImpact of Metabolic Syndrome and Its Severity On Microvascular ComplicationsMamad TrihatmowidjoyoNo ratings yet
- Statins and Beyond Concurrent Strategies For Prevention of Cardiovascular Disease in Patients WiDocument17 pagesStatins and Beyond Concurrent Strategies For Prevention of Cardiovascular Disease in Patients WiMamad TrihatmowidjoyoNo ratings yet
- Exercise Improves Cardiovascular Control in A Model of DislipidemiaDocument5 pagesExercise Improves Cardiovascular Control in A Model of DislipidemiaMamad TrihatmowidjoyoNo ratings yet
- Statins and Beyond Concurrent Strategies For Prevention of Cardiovascular Disease in Patients WiDocument17 pagesStatins and Beyond Concurrent Strategies For Prevention of Cardiovascular Disease in Patients WiMamad TrihatmowidjoyoNo ratings yet
- Glucose Prediction, IatrogeDocument6 pagesGlucose Prediction, IatrogeMamad TrihatmowidjoyoNo ratings yet
- Erythropoietin RequirementsDocument7 pagesErythropoietin RequirementsMamad TrihatmowidjoyoNo ratings yet
- The Anemia in Continuous Ambulatory Peritoneal DialysisDocument5 pagesThe Anemia in Continuous Ambulatory Peritoneal DialysisMamad TrihatmowidjoyoNo ratings yet
- Renal Association Clinical Practice Guideline On Anaemia of Chronic Kidney DiseaseDocument29 pagesRenal Association Clinical Practice Guideline On Anaemia of Chronic Kidney DiseasemelvinNo ratings yet
- 90-Article Text-458-1-10-20170910Document4 pages90-Article Text-458-1-10-20170910Mamad TrihatmowidjoyoNo ratings yet
- Latest Strategy in Renal Anemia Management in Peritoneal Dialysis PatientsDocument5 pagesLatest Strategy in Renal Anemia Management in Peritoneal Dialysis PatientsMamad TrihatmowidjoyoNo ratings yet
- The Spectrum of Red Blood CellDocument6 pagesThe Spectrum of Red Blood CellMamad TrihatmowidjoyoNo ratings yet
- 017791Document57 pages017791Miguel Chávez AmaroNo ratings yet
- Worksheet Guideline - AGREE AppraisalDocument2 pagesWorksheet Guideline - AGREE AppraisalRoel SamaNo ratings yet
- 09 - On Being A Scientist - Ethics PDFDocument83 pages09 - On Being A Scientist - Ethics PDFanita_shar29No ratings yet
- 09 - On Being A Scientist - Ethics PDFDocument83 pages09 - On Being A Scientist - Ethics PDFanita_shar29No ratings yet
- Role of Hyaluronic Acid and Laminin As Serum Markers For Predicting Significant Fibrosis in Patients With Chronic Hepatitis BDocument18 pagesRole of Hyaluronic Acid and Laminin As Serum Markers For Predicting Significant Fibrosis in Patients With Chronic Hepatitis BMamad TrihatmowidjoyoNo ratings yet
- 09 - On Being A Scientist - Ethics PDFDocument83 pages09 - On Being A Scientist - Ethics PDFanita_shar29No ratings yet
- 90-Article Text-458-1-10-20170910Document4 pages90-Article Text-458-1-10-20170910Mamad TrihatmowidjoyoNo ratings yet
- 09 - On Being A Scientist - Ethics PDFDocument83 pages09 - On Being A Scientist - Ethics PDFanita_shar29No ratings yet
- 09 - On Being A Scientist - Ethics PDFDocument83 pages09 - On Being A Scientist - Ethics PDFanita_shar29No ratings yet
- Mild Cognitive ImpairmentDocument1 pageMild Cognitive ImpairmentMamad TrihatmowidjoyoNo ratings yet
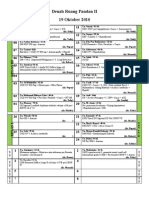
- Denah Ruang Pandan II Arsanto's Mode 101019Document2 pagesDenah Ruang Pandan II Arsanto's Mode 101019Mamad TrihatmowidjoyoNo ratings yet
- Tumor MarkersDocument54 pagesTumor MarkersMamad TrihatmowidjoyoNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- P2W1 Post Test MS Rle 8Document7 pagesP2W1 Post Test MS Rle 8Angel YN Patricio FlorentinoNo ratings yet
- Drug Name Drug Class Mechanism of Action Indications Contraindications Side Effects/ Adverse Effects Nursing ConsiderationDocument3 pagesDrug Name Drug Class Mechanism of Action Indications Contraindications Side Effects/ Adverse Effects Nursing ConsiderationKim SunooNo ratings yet
- Body FluidsDocument85 pagesBody FluidsShanta BharNo ratings yet
- Patient NCPDocument8 pagesPatient NCPlouie john abilaNo ratings yet
- Symmetry-Breaking of Animal CytokinesisDocument10 pagesSymmetry-Breaking of Animal CytokinesisLizbeth EspinosaNo ratings yet
- 0322008001Document160 pages0322008001Cherize G. MaliksiNo ratings yet
- Clinical Approach To Syncope in ChildrenDocument6 pagesClinical Approach To Syncope in ChildrenJahzeel Gacitúa Becerra100% (1)
- MebendazolDocument11 pagesMebendazolDiego SalvatierraNo ratings yet
- ENT NoseDocument18 pagesENT NosevkNo ratings yet
- Konsep Askep AntenatalDocument16 pagesKonsep Askep AntenatalBakul PariNo ratings yet
- Bell's Palsy - Symptoms and Causes - Mayo ClinicDocument6 pagesBell's Palsy - Symptoms and Causes - Mayo ClinicRoxan PacsayNo ratings yet
- Movicol Side EffectsDocument5 pagesMovicol Side EffectsniharjhatnNo ratings yet
- Manual of Infection Control Procedu PDFDocument365 pagesManual of Infection Control Procedu PDFanon_789115535100% (1)
- Assessment of Fetal Growth and DevelopmentDocument12 pagesAssessment of Fetal Growth and Developmentaracelisurat100% (1)
- Renal Function TestsDocument23 pagesRenal Function TestsKer YehunNo ratings yet
- The Seven Basic ChakrasDocument4 pagesThe Seven Basic ChakrasAlesha Rose100% (1)
- Schedule INDM202200111963 0.HomeLiteDocument51 pagesSchedule INDM202200111963 0.HomeLiteZeeshan HasanNo ratings yet
- 6.true Potato Seed - 0Document10 pages6.true Potato Seed - 0Almoustakbel AloustakbelNo ratings yet
- GONORRHEADocument8 pagesGONORRHEAFlorenceNo ratings yet
- Daily Life During The Black Death 01Document341 pagesDaily Life During The Black Death 01Rosie Davies100% (5)
- Dzinos MedicineDocument455 pagesDzinos MedicineCollen Lihaka100% (2)
- NCP PainDocument4 pagesNCP PainFlauros Ryu JabienNo ratings yet
- No Smoking in Public Places PolicyDocument3 pagesNo Smoking in Public Places PolicyCharlie PeinNo ratings yet
- NCM 101 Health AssessmentDocument7 pagesNCM 101 Health AssessmentCristoper Bodiongan100% (1)
- Freebirth LeseprobeDocument37 pagesFreebirth LeseprobedidibutterflyNo ratings yet
- Microbiology II - VirologyDocument8 pagesMicrobiology II - Virologyangel mintsNo ratings yet
- Vital PointsDocument3 pagesVital PointsAnand SudamaNo ratings yet
- Respiratory Drugs XL Chart 3Document2 pagesRespiratory Drugs XL Chart 3cdp1587100% (1)
- Gastroesophageal Reflux: Helping Your Baby: Patient and Family EducationDocument12 pagesGastroesophageal Reflux: Helping Your Baby: Patient and Family EducationAnita StefanieNo ratings yet
- Benguet State University: Drug StudyDocument2 pagesBenguet State University: Drug StudyKarla Karina Dela CruzNo ratings yet