You might also like
- Childhood Seized: Linguistic Considerations of the Effects of Epilepsy on Cognition in Children with Benign Childhood EpilepsyFrom EverandChildhood Seized: Linguistic Considerations of the Effects of Epilepsy on Cognition in Children with Benign Childhood EpilepsyNo ratings yet
- 2021 Biomed 001Document242 pages2021 Biomed 001CarlosNo ratings yet
- Echography and Doppler of the BrainFrom EverandEchography and Doppler of the BrainChiara RobbaNo ratings yet
- Central Nervous System Juvenile Xantogranuloma a cDocument96 pagesCentral Nervous System Juvenile Xantogranuloma a cAndrés WunderwaldNo ratings yet
- Chronic Immune-Mediated Demyelinating NeuropathiesDocument21 pagesChronic Immune-Mediated Demyelinating NeuropathiesArbey Aponte PuertoNo ratings yet
- Art. Demencia EegDocument15 pagesArt. Demencia EegMaría BarrettNo ratings yet
- Journal 2 BSPC SCI PublishedDocument16 pagesJournal 2 BSPC SCI PublishedDigambar PuriNo ratings yet
- KBG y ANKRD11 y ResonanciaDocument8 pagesKBG y ANKRD11 y ResonanciaAlberto Fernández JaénNo ratings yet
- Marino S Et Al, Longitudinal Analysis of Brain Atrophy in Alzheimer's Disease and Frontotemporal Dementia, 2019Document9 pagesMarino S Et Al, Longitudinal Analysis of Brain Atrophy in Alzheimer's Disease and Frontotemporal Dementia, 2019henryfv2010No ratings yet
- 10 31067-Acusaglik 1130277-2484596Document8 pages10 31067-Acusaglik 1130277-2484596Muhammet Hamit KarayılanNo ratings yet
- Automatic Detection of Genetic Diseases in Paediatric Age Using PupillometryDocument7 pagesAutomatic Detection of Genetic Diseases in Paediatric Age Using PupillometryIJRASETPublicationsNo ratings yet
- Color Density Spectral Array For Early EvaluationDocument7 pagesColor Density Spectral Array For Early EvaluationMunna KendreNo ratings yet
- Retinal Abnormatilites As A Diagnostic or Prognostic Marker of SchizophreniaDocument6 pagesRetinal Abnormatilites As A Diagnostic or Prognostic Marker of SchizophreniatratrNo ratings yet
- A Systematic Review On Etiology, Epidemiology, and Treatment of CPDocument10 pagesA Systematic Review On Etiology, Epidemiology, and Treatment of CPЯковлев АлександрNo ratings yet
- 2020 - Brain-First Versus Body-First Parkinson's Disease - A Multimodal Imaging Case-Control StudyDocument12 pages2020 - Brain-First Versus Body-First Parkinson's Disease - A Multimodal Imaging Case-Control StudyRaúl VerdugoNo ratings yet
- Extrapyramid SynDocument7 pagesExtrapyramid SynZahra Namika AiharaNo ratings yet
- Epilepsy and Brain LesionDocument9 pagesEpilepsy and Brain LesionPosadasLoezaJosueKarlaNo ratings yet
- 2012-Chatelle, Brain Injury, Brain-Computer Interfacing in Disorders of ConsciousnessDocument13 pages2012-Chatelle, Brain Injury, Brain-Computer Interfacing in Disorders of ConsciousnessImblnrNo ratings yet
- 2022 - BETROUNI Frontostriatal Subtype of MCI-PD, But Not The Posterior Cortical One, Is Associated With EEG AlterationsDocument12 pages2022 - BETROUNI Frontostriatal Subtype of MCI-PD, But Not The Posterior Cortical One, Is Associated With EEG AlterationsElisa FioraNo ratings yet
- MriCS EnglishDocument8 pagesMriCS Englishstefania caselleNo ratings yet
- 2helps2b ScoreDocument8 pages2helps2b ScoreGesael Passos Ferreira JuniorNo ratings yet
- Spect y ParkinsonDocument11 pagesSpect y ParkinsonJudith ButmanNo ratings yet
- Intelligence, Functioning, and Related Factors in Children With Cerebral PalsyDocument5 pagesIntelligence, Functioning, and Related Factors in Children With Cerebral PalsyAuliaRahmanNo ratings yet
- Journal AlzheimerDocument10 pagesJournal AlzheimerFaza KeumalasariNo ratings yet
- Fneur 11 00144Document22 pagesFneur 11 00144ilonaskorinNo ratings yet
- Clinical EEG and Neuroscience: Improving Alzheimer's Disease Diagnosis With Machine Learning TechniquesDocument7 pagesClinical EEG and Neuroscience: Improving Alzheimer's Disease Diagnosis With Machine Learning Techniqueskubranur karaNo ratings yet
- Arnaldi 2017Document10 pagesArnaldi 2017Jaime AguilarNo ratings yet
- Hippocampus's Volume Calculation On Coronal Slice's For Strengthening The Diagnosis of Alzheimer'sDocument10 pagesHippocampus's Volume Calculation On Coronal Slice's For Strengthening The Diagnosis of Alzheimer'sTELKOMNIKANo ratings yet
- 2011 PEDIATRIC HEAD Imaging GuidelinesDocument56 pages2011 PEDIATRIC HEAD Imaging GuidelinesElena BelonosovNo ratings yet
- Different Subtypes of DyskineticDocument8 pagesDifferent Subtypes of DyskineticMariana CarneiroNo ratings yet
- Abstracts / Journal of The Neurological Sciences 455 (2023) 121173 94Document2 pagesAbstracts / Journal of The Neurological Sciences 455 (2023) 121173 94Amin AminiNo ratings yet
- Nonvascular Retinal Imaging Markers of Preclinical Alzheimer S DiseaseDocument10 pagesNonvascular Retinal Imaging Markers of Preclinical Alzheimer S DiseaseMadhu C KNo ratings yet
- jpm-13-01411-v2Document15 pagesjpm-13-01411-v2Luluil MunirohNo ratings yet
- 1746-8094/published by Elsevier Ltd. Computer Aided Diagnosis System Using Deep Convolutional Neural Networks For ADHD SubtypesDocument10 pages1746-8094/published by Elsevier Ltd. Computer Aided Diagnosis System Using Deep Convolutional Neural Networks For ADHD SubtypesCésar SánchezNo ratings yet
- J of Neuroscience Research - 2022 - Valli - Neuroimaging of Rapid Eye Movement Sleep Behavior Disorder and Its Relation ToDocument20 pagesJ of Neuroscience Research - 2022 - Valli - Neuroimaging of Rapid Eye Movement Sleep Behavior Disorder and Its Relation ToKaramjot SinghNo ratings yet
- Safety and Efficacy Red Light For Alzheimer'sDocument9 pagesSafety and Efficacy Red Light For Alzheimer'sMonica SaavedraNo ratings yet
- Fnins 14 558532Document16 pagesFnins 14 558532anita putri effendiNo ratings yet
- Retinal ResponseDocument5 pagesRetinal ResponseguttersniperNo ratings yet
- Neuroimaging - Clinical ApplicationsDocument590 pagesNeuroimaging - Clinical ApplicationsIndera VyasNo ratings yet
- Cognitive Impairment in Parkinson's Disease: The Dual Syndrome HypothesisDocument14 pagesCognitive Impairment in Parkinson's Disease: The Dual Syndrome HypothesisRomina VelasquezNo ratings yet
- Cranial Manipulation Affects Cholinergic Pathway Gene Expression in Aged RatsDocument9 pagesCranial Manipulation Affects Cholinergic Pathway Gene Expression in Aged RatsTameemNo ratings yet
- 388.fullDocument8 pages388.fullMadhu CkNo ratings yet
- Past, Present and Future Alzheimer and OCTDocument38 pagesPast, Present and Future Alzheimer and OCTFernando lazzarettiNo ratings yet
- A Review of Diagnostic Techniques in The Differential Diagnosis of Epileptic and Nonepileptic SeizuresDocument34 pagesA Review of Diagnostic Techniques in The Differential Diagnosis of Epileptic and Nonepileptic Seizurestayfan1No ratings yet
- Deep CNN classifies depression from EEG with 95% accuracyDocument26 pagesDeep CNN classifies depression from EEG with 95% accuracyDhanalekshmi YedurkarNo ratings yet
- ACE MahuranathDocument9 pagesACE MahuranathStephanie Saavedra GomezNo ratings yet
- Neuro-Ophthalmologic Findings in Visual Snow Syndrome: Open AccessDocument7 pagesNeuro-Ophthalmologic Findings in Visual Snow Syndrome: Open AccessThomas ColodelNo ratings yet
- CNS Neuroscience Therapeutics - 2022 - Wang - Machine Learning Based on Optical Coherence Tomography Images as ADocument12 pagesCNS Neuroscience Therapeutics - 2022 - Wang - Machine Learning Based on Optical Coherence Tomography Images as AMadhu CkNo ratings yet
- REM Sleep Behaviour Disorder in Parkinson's Disease Is Associated With Specific Motor FeaturesDocument6 pagesREM Sleep Behaviour Disorder in Parkinson's Disease Is Associated With Specific Motor FeaturesPedro Moura GuedesNo ratings yet
- Diagnosing Chronic Glaucoma Using Watershed and Convolutional Neural Network-IJRASETDocument14 pagesDiagnosing Chronic Glaucoma Using Watershed and Convolutional Neural Network-IJRASETIJRASETPublicationsNo ratings yet
- Bab I Pendahuluan: Persistent Vegetative State in Head InjuryDocument17 pagesBab I Pendahuluan: Persistent Vegetative State in Head InjuryNindy Novela RitongaNo ratings yet
- Brain SPECT Imaging in Complex Psychiatric Cases: An Evidence-Based, Underutilized ToolDocument9 pagesBrain SPECT Imaging in Complex Psychiatric Cases: An Evidence-Based, Underutilized ToolMariaNo ratings yet
- AAN 2023 Day 1-2 Mind Next OriginalDocument21 pagesAAN 2023 Day 1-2 Mind Next Originalmpm8471No ratings yet
- Brainsci 12 00788 v3Document21 pagesBrainsci 12 00788 v3Krishna ArthiNo ratings yet
- jnc-200010-2Document7 pagesjnc-200010-2Nam LeeNo ratings yet
- Neurophysiological Recordings Improve The Accuracy of 2022 European JournalDocument6 pagesNeurophysiological Recordings Improve The Accuracy of 2022 European Journalcsepulveda10No ratings yet
- Remote and Longterm Selfmonitoring of Electroencephalographic and Noninvasive Measurable Variables at Home in Patients With Epilepsy EEGHOME Protocol For An Observational studyJMIR Research ProtocolsDocument12 pagesRemote and Longterm Selfmonitoring of Electroencephalographic and Noninvasive Measurable Variables at Home in Patients With Epilepsy EEGHOME Protocol For An Observational studyJMIR Research ProtocolsMiguel PalacioNo ratings yet
- Criteria For Defining Interictal Epileptiform Discharges in EEGDocument10 pagesCriteria For Defining Interictal Epileptiform Discharges in EEGMartha OktaviaNo ratings yet
- Choroideremia: Update On Clinical Features and Emerging TreatmentsDocument7 pagesChoroideremia: Update On Clinical Features and Emerging TreatmentsJocho NeavesNo ratings yet
- (IJCST-V11I2P10) :mr. V. Raghu Ram Chowdary, G. Tejaswini, E. Divya, K. Aditya, M. Varjan BabuDocument6 pages(IJCST-V11I2P10) :mr. V. Raghu Ram Chowdary, G. Tejaswini, E. Divya, K. Aditya, M. Varjan BabuEighthSenseGroupNo ratings yet
- Long-term voice and speech outcomes after CRTDocument7 pagesLong-term voice and speech outcomes after CRTDwi juliana DewiNo ratings yet
- Sal Men 2016Document9 pagesSal Men 2016Dwi juliana DewiNo ratings yet
- TON Agung Final (Autosaved)Document28 pagesTON Agung Final (Autosaved)Dwi juliana DewiNo ratings yet
- Sal Men 2016Document9 pagesSal Men 2016Dwi juliana DewiNo ratings yet
- Long-term voice and speech outcomes after CRTDocument7 pagesLong-term voice and speech outcomes after CRTDwi juliana DewiNo ratings yet
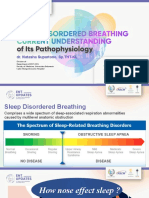
- Sesi 1 - Dr. Natasha SP - THT-KL - SDB Current Understanding of Its PathophysiologyDocument20 pagesSesi 1 - Dr. Natasha SP - THT-KL - SDB Current Understanding of Its PathophysiologyDwi juliana DewiNo ratings yet
- Lary 23467Document8 pagesLary 23467Dwi juliana DewiNo ratings yet
- Nasocardiac Reflex Bradycardia During Rhinological SurgeryDocument2 pagesNasocardiac Reflex Bradycardia During Rhinological SurgeryDwi juliana DewiNo ratings yet
- Consent for Publication of Figure ImageDocument1 pageConsent for Publication of Figure ImageDwi juliana DewiNo ratings yet
- Effect of Upper Airway Surgery On Heart Rate Variability in Patients With Obstructive Sleep Apnoea SyndromeDocument6 pagesEffect of Upper Airway Surgery On Heart Rate Variability in Patients With Obstructive Sleep Apnoea SyndromeDwi juliana DewiNo ratings yet
- Original Articles: X Deafness and Mental ToDocument7 pagesOriginal Articles: X Deafness and Mental ToDwi juliana DewiNo ratings yet
- Parasympathetic Overactivity in Patients With Nasal Septum DeformitiesDocument5 pagesParasympathetic Overactivity in Patients With Nasal Septum DeformitiesDwi juliana DewiNo ratings yet
- Cortical Visual Impairment inDocument11 pagesCortical Visual Impairment inDwi juliana DewiNo ratings yet
- Epidermal Nevus Syndrome WithDocument4 pagesEpidermal Nevus Syndrome WithDwi juliana DewiNo ratings yet
- Voice Handicap Index 2015Document1 pageVoice Handicap Index 2015Dwi juliana DewiNo ratings yet
- New Doc 2018-02-07 14.49.01-20180207144929 PDFDocument1 pageNew Doc 2018-02-07 14.49.01-20180207144929 PDFDwi juliana DewiNo ratings yet
- 1 Aka 57Document4 pages1 Aka 57Richard FadhilahNo ratings yet
- Common Mistakes in Legal EnglishDocument4 pagesCommon Mistakes in Legal Englishfreshbreeze_2006No ratings yet
- Export Processing Zone Authority vs. CHRDocument1 pageExport Processing Zone Authority vs. CHRKling KingNo ratings yet
- Magnetic Effects of Current PDFDocument32 pagesMagnetic Effects of Current PDFAdarshNo ratings yet
- Sources of Strength For Mental Wellness by Sheryl Boswell, Youth Mental Health Canada (YMHC)Document11 pagesSources of Strength For Mental Wellness by Sheryl Boswell, Youth Mental Health Canada (YMHC)Youth Mental Health CanadaNo ratings yet
- Conway - On Unsettleable Arithmetical ProblemsDocument8 pagesConway - On Unsettleable Arithmetical ProblemsfreafreafreaNo ratings yet
- Samsung Mobile: Market Share & Profitability in SmartphonesDocument15 pagesSamsung Mobile: Market Share & Profitability in SmartphonesTanmay WadhwaNo ratings yet
- SAP BusinessHubDocument384 pagesSAP BusinessHubNiravNo ratings yet
- 028 - Chapter 6 - L20 PDFDocument11 pages028 - Chapter 6 - L20 PDFRevathiNo ratings yet
- 15 January 2004 1st Lecture Herpetology ECOL 483/583 University of Arizona Spring 2004Document14 pages15 January 2004 1st Lecture Herpetology ECOL 483/583 University of Arizona Spring 2004andreaweiler1No ratings yet
- Examen Tema 3 Ingles EnzoDocument3 pagesExamen Tema 3 Ingles EnzoMartinEnzo GuerraNo ratings yet
- ISnack - Sec A Group6Document11 pagesISnack - Sec A Group6Avik BorahNo ratings yet
- Hypertext and Context in Text DevelopmentDocument3 pagesHypertext and Context in Text Developmentkiratuz1998No ratings yet
- English Profesional Nursering Book 2 PDFDocument35 pagesEnglish Profesional Nursering Book 2 PDFRed Millennium50% (2)
- Dawn Ullmann - ReferenceDocument1 pageDawn Ullmann - Referenceapi-418750957No ratings yet
- 2018 Sem 4Document8 pages2018 Sem 4shailesh latkarNo ratings yet
- Gle RubricDocument1 pageGle Rubricapi-207519916No ratings yet
- Injera Production and Export Business PlanDocument50 pagesInjera Production and Export Business PlanTumim84% (44)
- FLUID MECHANICS COURSEWORK QUESTIONSDocument6 pagesFLUID MECHANICS COURSEWORK QUESTIONSDelina TedrosNo ratings yet
- SyllabusDocument148 pagesSyllabusMadhu G. CNo ratings yet
- Julie Craven ResumeDocument3 pagesJulie Craven Resumeapi-469430606No ratings yet
- 3 Pehlke. Observations On The Historical Reliability of OT. SJT 56.1 (2013)Document22 pages3 Pehlke. Observations On The Historical Reliability of OT. SJT 56.1 (2013)Cordova Llacsahuache Leif100% (1)
- Fire Protection Focus for TunnelsDocument12 pagesFire Protection Focus for Tunnelsfrank100% (1)
- Element Six v. Novatek Et. Al.Document26 pagesElement Six v. Novatek Et. Al.PriorSmartNo ratings yet
- Prosthetics OrthoticsDocument9 pagesProsthetics OrthoticsSameeha AbbassNo ratings yet
- AtropineDocument6 pagesAtropineNiluh Komang Putri PurnamantiNo ratings yet
- DLL - All Subjects 2 - Q4 - W1 - D2Document9 pagesDLL - All Subjects 2 - Q4 - W1 - D2Catherine SeterraNo ratings yet
- 0310 Concrete Works en Rev ADocument17 pages0310 Concrete Works en Rev AJaime LandinginNo ratings yet
- MisOr Division Template in Action ResearchDocument14 pagesMisOr Division Template in Action ResearchAmorEmbone100% (2)
- Chapter-1 About BELDocument22 pagesChapter-1 About BELSHANKAR PRINTINGNo ratings yet
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (1)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionFrom EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionRating: 4 out of 5 stars4/5 (11)
- Fighting Words Devotional: 100 Days of Speaking Truth into the DarknessFrom EverandFighting Words Devotional: 100 Days of Speaking Truth into the DarknessRating: 5 out of 5 stars5/5 (6)
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsFrom EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsRating: 4.5 out of 5 stars4.5/5 (48)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (558)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- Insecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItFrom EverandInsecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (84)
- Call of the Wild: How We Heal Trauma, Awaken Our Own Power, and Use It For GoodFrom EverandCall of the Wild: How We Heal Trauma, Awaken Our Own Power, and Use It For GoodNo ratings yet
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationFrom EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationRating: 5 out of 5 stars5/5 (9)
- The Somatic Psychotherapy Toolbox: A Comprehensive Guide to Healing Trauma and StressFrom EverandThe Somatic Psychotherapy Toolbox: A Comprehensive Guide to Healing Trauma and StressNo ratings yet
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- Emotional Detox for Anxiety: 7 Steps to Release Anxiety and Energize JoyFrom EverandEmotional Detox for Anxiety: 7 Steps to Release Anxiety and Energize JoyRating: 5 out of 5 stars5/5 (6)
- The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk: Key Takeaways, Summary & AnalysisFrom EverandThe Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (2)