You might also like
- 1 s2.0 S2590041221000039 MainDocument2 pages1 s2.0 S2590041221000039 MainMa No LoNo ratings yet
- Annals of Clinical Medicine and Research: Pulmonary Cavitation Post-COVID-19 Pneumonia: A CaseDocument3 pagesAnnals of Clinical Medicine and Research: Pulmonary Cavitation Post-COVID-19 Pneumonia: A CaseChavdarNo ratings yet
- Plasma Cytokine Profile On Admission Related To Aetiology in Community Acquired PneumoniaDocument9 pagesPlasma Cytokine Profile On Admission Related To Aetiology in Community Acquired Pneumoniahusni gunawanNo ratings yet
- Bacterial and Viral Infection in Patients Hospitalized For Acute Exacerbation of Chronic Obstructive Pulmonary Disease Implication For Antimicrobial-1Document10 pagesBacterial and Viral Infection in Patients Hospitalized For Acute Exacerbation of Chronic Obstructive Pulmonary Disease Implication For Antimicrobial-1Ayu SusiyanthiNo ratings yet
- Post Covid-19 Organizing Pneumonia Case Series For 6 Patients With post-COVID Interstitial Lung DiseaseDocument4 pagesPost Covid-19 Organizing Pneumonia Case Series For 6 Patients With post-COVID Interstitial Lung DiseaseKhangNo ratings yet
- Pneumothorax in Active Pulmonary Tuberculosis: Resurgence of An Old Complication?Document5 pagesPneumothorax in Active Pulmonary Tuberculosis: Resurgence of An Old Complication?M Tata SuhartaNo ratings yet
- 2007 Diagnostic Strategies in Nosocomial PneumoniaDocument6 pages2007 Diagnostic Strategies in Nosocomial PneumoniaIvana Daniela BelloNo ratings yet
- PIIS0012369215421269Document2 pagesPIIS0012369215421269chicyNo ratings yet
- Organizing Pneumonia Following Covid19 PneumoniaDocument4 pagesOrganizing Pneumonia Following Covid19 PneumoniaKhangNo ratings yet
- Bronchoscopy in Critically Ill COVID-19 Patients - Findings, Microbiological Profile, and CoinfectionDocument5 pagesBronchoscopy in Critically Ill COVID-19 Patients - Findings, Microbiological Profile, and CoinfectionJeisson Osorio TrujilloNo ratings yet
- Coexistent Pulm Crypto & Sarcoidosis 2020Document6 pagesCoexistent Pulm Crypto & Sarcoidosis 2020Eashaa KumarNo ratings yet
- Estudo StopcovidDocument11 pagesEstudo StopcoviddravlamfNo ratings yet
- Difficulties in Diagnosis of Psittacosis or Ornithosis: A Case ReportDocument4 pagesDifficulties in Diagnosis of Psittacosis or Ornithosis: A Case ReportYusrinabillaNo ratings yet
- Positive Chest CT Features in Patients With COVID-19 Pneumonia and Negative Real-Time Polymerase Chain Reaction TestDocument16 pagesPositive Chest CT Features in Patients With COVID-19 Pneumonia and Negative Real-Time Polymerase Chain Reaction TestHector MarrufoNo ratings yet
- DeteksionDocument9 pagesDeteksionkasandraharahapNo ratings yet
- Respiratory Medicine Case ReportsDocument8 pagesRespiratory Medicine Case ReportsdiahNo ratings yet
- Jurnal Deteksi Cendawan DimorfikDocument13 pagesJurnal Deteksi Cendawan DimorfikIkha UdmalasariNo ratings yet
- Patogenos BacterianosDocument7 pagesPatogenos BacterianosHumberto QuinteroNo ratings yet
- Pneumonia: V. Mandang, M.DDocument44 pagesPneumonia: V. Mandang, M.DMeggy SumarnoNo ratings yet
- UyutdgfDocument5 pagesUyutdgfswabrijNo ratings yet
- Pneumothorax in Critically COVID-19 Patients With Mechanical VentilationDocument5 pagesPneumothorax in Critically COVID-19 Patients With Mechanical VentilationNadyaNo ratings yet
- Jurnal CovidDocument15 pagesJurnal CovidFitriani NurFadillahNo ratings yet
- Staphylococcus Aureus Bacteremic Pneumonia: Differences Between Community and Nosocomial AcquisitionDocument7 pagesStaphylococcus Aureus Bacteremic Pneumonia: Differences Between Community and Nosocomial AcquisitionrisnaNo ratings yet
- CT Features of Community-Acquired Pneumonia at The Emergency DepartmentDocument8 pagesCT Features of Community-Acquired Pneumonia at The Emergency DepartmentpachomdNo ratings yet
- Nej M 199508243330802Document7 pagesNej M 199508243330802Pieter JohnyNo ratings yet
- Review: Atypical Pathogen Infection in Community-Acquired PneumoniaDocument7 pagesReview: Atypical Pathogen Infection in Community-Acquired PneumoniaDebi SusantiNo ratings yet
- Procalcitonin 6Document11 pagesProcalcitonin 6zivl1984No ratings yet
- Valente Acosta2020Document4 pagesValente Acosta2020Andres TameNo ratings yet
- PCT, Crpjomb-36-122Document5 pagesPCT, Crpjomb-36-122muhammadNo ratings yet
- 1 s2.0 S1198743X18308565 MainDocument6 pages1 s2.0 S1198743X18308565 MainYulia Niswatul FauziyahNo ratings yet
- Macrolide Therapy in Cryptogenic Organizing Pneumonia: A Case Report and Literature ReviewDocument7 pagesMacrolide Therapy in Cryptogenic Organizing Pneumonia: A Case Report and Literature Reviewdicky wahyudiNo ratings yet
- 2017 Fosfato de CalcioDocument9 pages2017 Fosfato de CalcioAngy ÑacatoNo ratings yet
- Value of Pneumococcal PCR in Respiratory Samples For Exclusion of PneumococcalDocument5 pagesValue of Pneumococcal PCR in Respiratory Samples For Exclusion of PneumococcalWilliam BarreraNo ratings yet
- Procalcitonin 2Document6 pagesProcalcitonin 2zivl1984No ratings yet
- Ijcr 4045 20230703 V1Document3 pagesIjcr 4045 20230703 V1haryatiNo ratings yet
- m20 2003 PDFDocument14 pagesm20 2003 PDFTobias Ernesto Rivas GarciaNo ratings yet
- OutDocument12 pagesOutYasminNo ratings yet
- Jurnal 20Document5 pagesJurnal 20Ahmad Fari Arief LopaNo ratings yet
- Chest CT Imaging Features of COVID-19-Related Pulmonary Fibrosis: A Case ReportDocument4 pagesChest CT Imaging Features of COVID-19-Related Pulmonary Fibrosis: A Case ReportharryNo ratings yet
- 7 Clinical Characteristics00196 FinalDocument9 pages7 Clinical Characteristics00196 FinalDarveen VijayanNo ratings yet
- Pneumonia 3Document8 pagesPneumonia 3furqan92No ratings yet
- Correlations of CT Scan With High-Sensitivity C-ReDocument5 pagesCorrelations of CT Scan With High-Sensitivity C-ReAnthony ChristantoNo ratings yet
- Hunter - VAP - Postgrad Med J-2006 (Bakteri Penyebab VAP Terbanyak)Document8 pagesHunter - VAP - Postgrad Med J-2006 (Bakteri Penyebab VAP Terbanyak)Irfany Nurul HamidNo ratings yet
- Respiratory Medicine CME: Lancelot Mark Pinto, Arpan Chandrakant Shah, Kushal Dipakkumar Shah, Zarir Farokh UdwadiaDocument3 pagesRespiratory Medicine CME: Lancelot Mark Pinto, Arpan Chandrakant Shah, Kushal Dipakkumar Shah, Zarir Farokh UdwadiaLintang SuroyaNo ratings yet
- Tofacitinib in Patients Hospitalized With Covid-19 PneumoniaDocument11 pagesTofacitinib in Patients Hospitalized With Covid-19 PneumoniaRenato MoreiraNo ratings yet
- Hemoptysis Following A Chronic IllnessDocument2 pagesHemoptysis Following A Chronic IllnessDhiya RahadianNo ratings yet
- Test 1 Pne 01Document8 pagesTest 1 Pne 01Zdravko SavićNo ratings yet
- Ejifcc 2022 Vol 33 No 2Document139 pagesEjifcc 2022 Vol 33 No 2Georgiana Daniela DragomirNo ratings yet
- Acremonium Pneumonia: Case Report and Literature Review: TanaffosDocument5 pagesAcremonium Pneumonia: Case Report and Literature Review: TanaffosNurmawati AtNo ratings yet
- Pneumocystis PneumoniaDocument16 pagesPneumocystis PneumoniaMaría Luisa MantillaNo ratings yet
- Pneumonia Panel GuidelineDocument8 pagesPneumonia Panel Guidelineilham perdiansyahNo ratings yet
- Organising Pneumonia Manifesting As A Late Phase Complication of COVID-19Document3 pagesOrganising Pneumonia Manifesting As A Late Phase Complication of COVID-19KhangNo ratings yet
- Serum Procalcitonin in Pneumococcal Pneumonia in Children: M. Korppi, S. RemesDocument5 pagesSerum Procalcitonin in Pneumococcal Pneumonia in Children: M. Korppi, S. Remesmr_curiousityNo ratings yet
- Pneumonia in Critical Patients - KARTIKADocument29 pagesPneumonia in Critical Patients - KARTIKAKartika JuwitaNo ratings yet
- Nac 2017Document18 pagesNac 2017Nataly CortesNo ratings yet
- Pulmonary Tuberculosis Journal ResearchDocument30 pagesPulmonary Tuberculosis Journal ResearchArfania LailyNo ratings yet
- Nebulized Colistin in The Treatment of Pneumonia Due To Multidrug-Resistant Acinetobacter Baumannii and Pseudomonas AeruginosaDocument4 pagesNebulized Colistin in The Treatment of Pneumonia Due To Multidrug-Resistant Acinetobacter Baumannii and Pseudomonas AeruginosaPhan Tấn TàiNo ratings yet
- Basic Concepts On Communityacquired Bacterial Pneumonia in PediatricsDocument6 pagesBasic Concepts On Communityacquired Bacterial Pneumonia in PediatricsJesselle LasernaNo ratings yet
- Rituximab - Pulmonary ToxicityDocument10 pagesRituximab - Pulmonary ToxicityRK SpartacusNo ratings yet
- PROBLEM 4.156: SolutionDocument11 pagesPROBLEM 4.156: SolutionYennifer OrtegozaNo ratings yet
- Siam Park: Benjamin StoimenovDocument33 pagesSiam Park: Benjamin StoimenovMichael WyrschNo ratings yet
- Using The Behringer FCB1010 With The TC GDocument6 pagesUsing The Behringer FCB1010 With The TC GLuis UríaNo ratings yet
- 1-S2.0-S1877042812020769-Main - Rail LogisticDocument4 pages1-S2.0-S1877042812020769-Main - Rail LogisticDodi Julianto فاصلNo ratings yet
- Lab 4 Enzymes and The Catalase LabDocument18 pagesLab 4 Enzymes and The Catalase LabAmy Hollingsworth100% (1)
- Melendrez - Jhoana - Laboratory 2Document3 pagesMelendrez - Jhoana - Laboratory 2JHOANA MELENDREZNo ratings yet
- Final Natural System of Success 2018Document3 pagesFinal Natural System of Success 2018Shailesh PillaiNo ratings yet
- Canon Eos 300d Service ManualDocument109 pagesCanon Eos 300d Service ManualEnrique RichardNo ratings yet
- Product Data: Hempel's Light Primer 45550Document2 pagesProduct Data: Hempel's Light Primer 45550satish rongalaNo ratings yet
- 10 Philippines Herbal Medicine Approved by DOH (Pharmacology Topic)Document10 pages10 Philippines Herbal Medicine Approved by DOH (Pharmacology Topic)Neisha Halil VillarealNo ratings yet
- NASA Facts Lightning Protection For NASA's Next Generation SpacecraftDocument2 pagesNASA Facts Lightning Protection For NASA's Next Generation SpacecraftBob AndrepontNo ratings yet
- Assignment-CA SIC2002Document6 pagesAssignment-CA SIC2002Baginda RamleeNo ratings yet
- Aahar 2024 Hallwise List of ParticipantsDocument102 pagesAahar 2024 Hallwise List of ParticipantsDeepak J SharmaNo ratings yet
- Camouflage Yourself and Individual EquipmentDocument16 pagesCamouflage Yourself and Individual EquipmentInficeman100% (1)
- Elaboration of Actual FreedomDocument197 pagesElaboration of Actual FreedomJustine50% (2)
- Electric SignalsDocument29 pagesElectric Signalsyttan1116No ratings yet
- Navmc 3500 - 44a PT 4Document200 pagesNavmc 3500 - 44a PT 4taylorNo ratings yet
- Touchstone 1 - 2nd Edition - Quiz Unit 12Document2 pagesTouchstone 1 - 2nd Edition - Quiz Unit 12syllindacardosoNo ratings yet
- The Calendar From The Beginning To The EndDocument73 pagesThe Calendar From The Beginning To The EndPetko Nikolic Vidusa100% (4)
- Swathi PDFDocument2 pagesSwathi PDFPalaniappan GurusamyNo ratings yet
- Acupuncture. Does It Works?Document6 pagesAcupuncture. Does It Works?John ThunderNo ratings yet
- Artikel Jurnal - Nur Alimul Hakim - 42117055-5Document12 pagesArtikel Jurnal - Nur Alimul Hakim - 42117055-5cinta burungNo ratings yet
- Ags PrimusDocument1 pageAgs PrimusGireesh HegdeNo ratings yet
- Exercise 1 - TVM & Equivalence 2.0Document5 pagesExercise 1 - TVM & Equivalence 2.0Bayu PurnamaNo ratings yet
- Dkg-329 User ManualDocument43 pagesDkg-329 User ManualKỹ Sư TđhNo ratings yet
- Aluminium Rail CoachDocument7 pagesAluminium Rail CoachdselvakuuNo ratings yet
- Greentech Profile 2Document16 pagesGreentech Profile 2Benjie AlfelorNo ratings yet
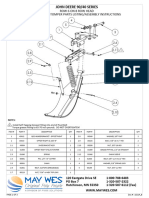
- JD 90 - 40 Rows 3 - 6 On 8 RowDocument7 pagesJD 90 - 40 Rows 3 - 6 On 8 Rowalaynnastaabx786No ratings yet
- Fema 450Document752 pagesFema 450Pitulice Silvia100% (1)
- Report On Automatic Gear Shift For 2wheelersDocument92 pagesReport On Automatic Gear Shift For 2wheelersDeepak ChaurasiaNo ratings yet