You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team Building ActivitiesDocument7 pagesTeam Building ActivitiesInsaneNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- EY Performance Control EnvironmentDocument10 pagesEY Performance Control EnvironmentIndra WantoNo ratings yet
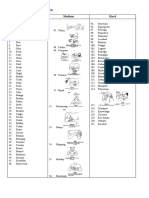
- Spelling Bee WordsDocument6 pagesSpelling Bee WordsSOLEHAH BINTI IBRAHIM MoeNo ratings yet
- The Seven Laws of The Universe (Ebook)Document4 pagesThe Seven Laws of The Universe (Ebook)April Capa100% (1)
- Laser SettingsDocument1 pageLaser SettingsPedro Mendoza BarriosNo ratings yet
- Al Waqiah PDF To Excel PDFDocument4 pagesAl Waqiah PDF To Excel PDFRehman KhanNo ratings yet
- Coding Theory BookDocument243 pagesCoding Theory BookjHexstNo ratings yet
- Promoting Fairness in Mobile Ad Hoc NetworksDocument4 pagesPromoting Fairness in Mobile Ad Hoc NetworksBONFRINGNo ratings yet
- Unit Iv: Data Reception AND Data ProductsDocument23 pagesUnit Iv: Data Reception AND Data ProductsDivya PurushothamanNo ratings yet
- A Theory of EmotionDocument12 pagesA Theory of Emotionmihaela irofteNo ratings yet
- Relativistic Doppler Effect and The Principle of Relativity: W. EngelhardtDocument21 pagesRelativistic Doppler Effect and The Principle of Relativity: W. EngelhardtThebe AlfarisiNo ratings yet
- Online Banking - WikipediaDocument39 pagesOnline Banking - WikipediaAjay RathodNo ratings yet
- Cryogenic TechnologyDocument12 pagesCryogenic TechnologyALOKSRKNo ratings yet
- Overview of Pubic Administration An ActiDocument9 pagesOverview of Pubic Administration An ActiShaniah VilleNo ratings yet
- Windows Mobile Programming Usinb Basic4ppcDocument30 pagesWindows Mobile Programming Usinb Basic4ppcmeeraneela0808No ratings yet
- JPCL Wastewater Ebook2013Document35 pagesJPCL Wastewater Ebook2013Alex PazmiñoNo ratings yet
- GEST 79 76 Edition 4Document26 pagesGEST 79 76 Edition 4روشان فاطمة روشانNo ratings yet
- Fes TBT Mobile CraneDocument1 pageFes TBT Mobile CraneMohammed AtefNo ratings yet
- BATL061Document20 pagesBATL061Roxana TroacaNo ratings yet
- Louisiana sb271 EnactedDocument19 pagesLouisiana sb271 Enactedapi-344608330No ratings yet
- 100 Years of Ammonia Synthesis Technology: Ib DybkjærDocument10 pages100 Years of Ammonia Synthesis Technology: Ib DybkjærGrootNo ratings yet
- Prospect of Tourism in RanchiDocument27 pagesProspect of Tourism in RanchiManish M. Surin0% (1)
- BRC0202 012038MDocument4 pagesBRC0202 012038MYarn HeartNo ratings yet
- Learner'S Packet (Leap: Learning Area Grade LevelDocument4 pagesLearner'S Packet (Leap: Learning Area Grade LeveljamNo ratings yet
- Why Is Smoking Harmful in Pregnancy?Document2 pagesWhy Is Smoking Harmful in Pregnancy?SitaNo ratings yet
- Heckler & Kock - G3 Armorer's ManualDocument50 pagesHeckler & Kock - G3 Armorer's ManualRicardo C TorresNo ratings yet
- Past Perfect Continuous Tense - EnglishClubDocument3 pagesPast Perfect Continuous Tense - EnglishClubidahashimNo ratings yet
- Modernism NotesDocument10 pagesModernism NotesKonstantina ToulaNo ratings yet
- Nokia 6.1 Plus (Black, 64 GB) : Grand Total 14999.00Document1 pageNokia 6.1 Plus (Black, 64 GB) : Grand Total 14999.00Udit PandeyNo ratings yet
- PNRC List of ArticlesDocument4 pagesPNRC List of Articlesruchikakaushal1910No ratings yet