You might also like
- Weekly 14 January - 20 Jan 2018 IGD 1Document22 pagesWeekly 14 January - 20 Jan 2018 IGD 1Alfonso AnggriawanNo ratings yet
- Laporan Mingguan: SMF Obstetri Dan GinekologiDocument20 pagesLaporan Mingguan: SMF Obstetri Dan GinekologiDivika ShilvanaNo ratings yet
- MCQ Notes Dr.nadineنساDocument381 pagesMCQ Notes Dr.nadineنساAhmed MansourNo ratings yet
- Laporan Mingguan: SMF Obstetri Dan GinekologiDocument19 pagesLaporan Mingguan: SMF Obstetri Dan GinekologiDivika ShilvanaNo ratings yet
- Common Hospital Abbreviations12Document4 pagesCommon Hospital Abbreviations12marykNo ratings yet
- Maternal and Child NursingsDocument16 pagesMaternal and Child NursingsQueennie Hafsah K. PangandamanNo ratings yet
- B3Y5G3 O - G - With AnswersDocument4 pagesB3Y5G3 O - G - With AnswersZeke EdgeNo ratings yet
- Common Hospital Abbreviations12Document5 pagesCommon Hospital Abbreviations12Christelle PoNo ratings yet
- Ospe Exam O&gDocument43 pagesOspe Exam O&gNabilah Mohammad KhalisNo ratings yet
- Patient's Name: Pedia: Mother's Name: OB-Gyne: Room: Blood Type: Date of Birth: JI In-Charge: Time of Birth: Admitting Notes I. General DataDocument2 pagesPatient's Name: Pedia: Mother's Name: OB-Gyne: Room: Blood Type: Date of Birth: JI In-Charge: Time of Birth: Admitting Notes I. General DataColeen NeyraNo ratings yet
- Common Hospital AbbreviationsDocument4 pagesCommon Hospital AbbreviationsKarlalots CasiñoNo ratings yet
- Final Obgn HandoutDocument36 pagesFinal Obgn HandoutAhmad Faizul AbdrahmansazliNo ratings yet
- B4Y5G3 O - G - With AnswersDocument6 pagesB4Y5G3 O - G - With AnswersZeke EdgeNo ratings yet
- ABORTION AND ECTOPIC PREGNANCY 2nd LecDocument9 pagesABORTION AND ECTOPIC PREGNANCY 2nd LecDominion OgochukwuNo ratings yet
- Complications of 3 Stage of LabourDocument17 pagesComplications of 3 Stage of LabourshravaniNo ratings yet
- Tugas Bahasa Inggris 2Document5 pagesTugas Bahasa Inggris 2Wida YatiNo ratings yet
- Operating Theatre Report: Tuesday, April 23 2019Document54 pagesOperating Theatre Report: Tuesday, April 23 2019pogimudaNo ratings yet
- Saudi Board Exam 2015: These Answers Are Mine, They May Be Right, May Be WrongDocument22 pagesSaudi Board Exam 2015: These Answers Are Mine, They May Be Right, May Be WrongAloah122346No ratings yet
- Audit Ahad DepanDocument16 pagesAudit Ahad DepanNorfaizah FxNo ratings yet
- CBA 8 MCQ Compilation 2020Document17 pagesCBA 8 MCQ Compilation 2020Sadia YousafNo ratings yet
- Soif NSDocument4 pagesSoif NSIlmiah Program studi ObginNo ratings yet
- TetekDocument4 pagesTetekasoly giovanoNo ratings yet
- HIDDENDocument12 pagesHIDDENEdvansHenryNo ratings yet
- Gyna Full QDocument43 pagesGyna Full QMohammed Isa HomidatNo ratings yet
- Medical ExamDocument38 pagesMedical Examchikinlam900No ratings yet
- Edit - Daily OK IGD HIL 06.11.2019Document7 pagesEdit - Daily OK IGD HIL 06.11.2019Inez WijayaNo ratings yet
- 0010obstetric ClerkingDocument4 pages0010obstetric ClerkingAnivasa KabirNo ratings yet
- Saudimedstudent 1DEC SMLEDocument45 pagesSaudimedstudent 1DEC SMLEIndrajit BaruaNo ratings yet
- Ob NotesDocument63 pagesOb NotesRoger AcasusoNo ratings yet
- Abortion PresentationDocument46 pagesAbortion PresentationJhong Xyrus67% (3)
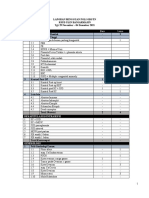
- Obstetri: Laporan Mingguan Poli Obgyn Rsud Ulin Banjarmasin Tgl. 29 November - 04 Desember 2021Document4 pagesObstetri: Laporan Mingguan Poli Obgyn Rsud Ulin Banjarmasin Tgl. 29 November - 04 Desember 2021aldoNo ratings yet
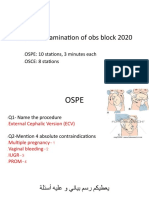
- Practical Examination of Obs Block 2020Document11 pagesPractical Examination of Obs Block 2020Female calmNo ratings yet
- Bid-Twice A Day BCG - Bacillus Calmette Guerine BM - Bowel Movement Bow - Bag of Water Baiae - Bronchial Asthma in Ba - Bronchial Asthma BPN - BronchopneumoniaDocument8 pagesBid-Twice A Day BCG - Bacillus Calmette Guerine BM - Bowel Movement Bow - Bag of Water Baiae - Bronchial Asthma in Ba - Bronchial Asthma BPN - BronchopneumoniaJohn Paolo OcampoNo ratings yet
- Obs and Gyn 6 Year Final Exam / 2012: A. PcosDocument13 pagesObs and Gyn 6 Year Final Exam / 2012: A. PcosNashaat H. AlshawabkehNo ratings yet
- Medical Case Write UpDocument11 pagesMedical Case Write UpJang Abd MutalibNo ratings yet
- 6th Awn 2019Document7 pages6th Awn 2019Mohammad AlrefaiNo ratings yet
- Exam MohemDocument7 pagesExam Mohemnada elfarraNo ratings yet
- Syifaa'.Wani - Shera.Achik - Syaa.Alin - Anis.Fatin - Yaya. THE 9 X-VIBRANT2017Document23 pagesSyifaa'.Wani - Shera.Achik - Syaa.Alin - Anis.Fatin - Yaya. THE 9 X-VIBRANT2017Nadhirah ZulkifliNo ratings yet
- DR - Ario - Kehamilan DGN Penyulit 4 (Perdarahan Dalam Kehamilan)Document40 pagesDR - Ario - Kehamilan DGN Penyulit 4 (Perdarahan Dalam Kehamilan)Lisa Raihan LutfiaNo ratings yet
- Lecture-25 Cesarean SectionDocument21 pagesLecture-25 Cesarean SectionMadhu Sudhan PandeyaNo ratings yet
- Laporan Mingguan: SMF Obstetri Dan GinekologiDocument13 pagesLaporan Mingguan: SMF Obstetri Dan GinekologiSitha MahendrataNo ratings yet
- Yulia AFDocument12 pagesYulia AFIlmiah Program studi ObginNo ratings yet
- Role of Us in Obstetric ProblemsDocument21 pagesRole of Us in Obstetric ProblemstadeleNo ratings yet
- Prelim 2020 Paper 1Document4 pagesPrelim 2020 Paper 1rajendra panwarNo ratings yet
- 009obs and Gynae History TakingDocument13 pages009obs and Gynae History TakingAnivasa KabirNo ratings yet
- 009obs and Gynae History TakingDocument13 pages009obs and Gynae History TakingkbNo ratings yet
- Ob Reviewer (Side Notes) : Most Common (Leading) Causes of Maternal Death Sa Pilipinas: 2019Document4 pagesOb Reviewer (Side Notes) : Most Common (Leading) Causes of Maternal Death Sa Pilipinas: 2019k76pk6brv9No ratings yet
- Artigo Gravidez EctópicaDocument2 pagesArtigo Gravidez EctópicaKevin UchoaNo ratings yet
- QuestionsDocument18 pagesQuestionsSalmonella TyphiNo ratings yet
- Common AbbreviationDocument4 pagesCommon AbbreviationKyla Marie TejadaNo ratings yet
- Selection SurgeryDocument11 pagesSelection SurgeryRawanNo ratings yet
- Ingles Medicina IIDocument22 pagesIngles Medicina IIxamiracastroalcantaraNo ratings yet
- Obstetrics Emergencies in Primary Care 4.3.20Document11 pagesObstetrics Emergencies in Primary Care 4.3.20hakimahsNo ratings yet
- Fatal Civil Aircraft Accidents: Their Medical and Pathological InvestigationFrom EverandFatal Civil Aircraft Accidents: Their Medical and Pathological InvestigationNo ratings yet
- Spontaneous Preterm Birth - Pathogenesis - UpToDateDocument20 pagesSpontaneous Preterm Birth - Pathogenesis - UpToDateAyu Dyah PrimaningrumNo ratings yet
- Progesterone Supplementation To Reduce The Risk of Spontaneous Preterm Labor and Birth - UpToDateDocument24 pagesProgesterone Supplementation To Reduce The Risk of Spontaneous Preterm Labor and Birth - UpToDateAyu Dyah PrimaningrumNo ratings yet
- Incidence and Mortality of The Preterm Infant - UpToDateDocument29 pagesIncidence and Mortality of The Preterm Infant - UpToDateAyu Dyah PrimaningrumNo ratings yet
- Template New Report Akreta Update EropaDocument1 pageTemplate New Report Akreta Update EropaAyu Dyah PrimaningrumNo ratings yet
- AUB M Ec Hiperplasia Endometrium - Id.enDocument2 pagesAUB M Ec Hiperplasia Endometrium - Id.enAyu Dyah PrimaningrumNo ratings yet
- Constipation in PregnancyDocument32 pagesConstipation in PregnancyAyu Dyah PrimaningrumNo ratings yet
- Weekly RK 3-8 May 2021 Edit 1Document2 pagesWeekly RK 3-8 May 2021 Edit 1Ayu Dyah PrimaningrumNo ratings yet
- Beta HCG in RPOCDocument1 pageBeta HCG in RPOCAyu Dyah PrimaningrumNo ratings yet
- RPOC Treatment Surgery Vs MTXDocument2 pagesRPOC Treatment Surgery Vs MTXAyu Dyah PrimaningrumNo ratings yet
- "Nausicaa" Compression SutureDocument14 pages"Nausicaa" Compression SutureAyu Dyah PrimaningrumNo ratings yet
- Abortion Procedures During First, Second and Third TrimesterDocument2 pagesAbortion Procedures During First, Second and Third TrimesterJhon Jade PalagtiwNo ratings yet
- Cerclaje en Embarazo GemelarDocument9 pagesCerclaje en Embarazo GemelarSofía Contreras SalazarNo ratings yet
- PolyhydramniosDocument5 pagesPolyhydramniosPATRICIA SAN PEDRONo ratings yet
- PNDTA Technical Aspects 2012Document69 pagesPNDTA Technical Aspects 2012arunmorayNo ratings yet
- EABDocument12 pagesEABAr Kethees WaranNo ratings yet
- 137-Article Text-304-1-10-20200309Document7 pages137-Article Text-304-1-10-20200309agustina silalahiNo ratings yet
- PDFDocument5 pagesPDFKinjal VasavaNo ratings yet
- Sample Nursing QuestionsDocument4 pagesSample Nursing QuestionsZhy CaluzaNo ratings yet
- Study On Postnatal Care in A Tertiary Care Hospital in Eastern India and The RealityDocument7 pagesStudy On Postnatal Care in A Tertiary Care Hospital in Eastern India and The RealityTanishka JohriNo ratings yet
- Breech Presentation-Muhammad NzarDocument26 pagesBreech Presentation-Muhammad NzarRaman Khdr QaladzayNo ratings yet
- The Influence of PCIM Health Education Module On The Self-Efficacy of Primiparous in Taking Care of Newborn in Haharu, East SumbaDocument12 pagesThe Influence of PCIM Health Education Module On The Self-Efficacy of Primiparous in Taking Care of Newborn in Haharu, East Sumbamutia aNo ratings yet
- Diabetes in Pregnancy: Supervisor: DR Rathimalar By: DR Ashwini Arumugam & DR Laily MokhtarDocument21 pagesDiabetes in Pregnancy: Supervisor: DR Rathimalar By: DR Ashwini Arumugam & DR Laily MokhtarHarleyquinn96 DrNo ratings yet
- Obstetric Nursing Practice Test Part 1Document10 pagesObstetric Nursing Practice Test Part 1yanee06No ratings yet
- Stages of Labor.......Document3 pagesStages of Labor.......Jowen AngeloNo ratings yet
- Daftar Pustaka MiomaDocument2 pagesDaftar Pustaka Mioma2tialawiNo ratings yet
- Critical Appraisal PROGNOSIS Jurnal ReadingDocument5 pagesCritical Appraisal PROGNOSIS Jurnal Readingsiekasmat upaNo ratings yet
- Prolonged PregnancyDocument45 pagesProlonged PregnancyReshmi S ChellappanNo ratings yet
- A Literature Review of Midwifery-Led Care in Reducing Labor and Birth InterventionsDocument14 pagesA Literature Review of Midwifery-Led Care in Reducing Labor and Birth Interventionsradilla syafitriNo ratings yet
- Cardiotocograph (CTG) Interpretation and ResponseDocument23 pagesCardiotocograph (CTG) Interpretation and ResponseAndi Farid ANo ratings yet
- Factors Associated With Hypertensive Pregnancy Syndrome - Analysis Multiple in Hierarchical ModelsDocument8 pagesFactors Associated With Hypertensive Pregnancy Syndrome - Analysis Multiple in Hierarchical ModelsWeslley FerreiraNo ratings yet
- Cesearean Section FinalDocument62 pagesCesearean Section Finalsanthiyasandy75% (4)
- What Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and UterineDocument18 pagesWhat Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and Uterineمحمداحمد محمدنور ابايزيدNo ratings yet
- Schoolarship Exam MCQsDocument12 pagesSchoolarship Exam MCQsSaber AlasmarNo ratings yet
- Acog Practice Bulletin Summary: Gestational Hypertension and PreeclampsiaDocument4 pagesAcog Practice Bulletin Summary: Gestational Hypertension and PreeclampsiaKevin CasavilcaNo ratings yet
- Face and Brow Presentations in LaborDocument6 pagesFace and Brow Presentations in LabordenekeNo ratings yet
- Syekh Yusuf Gowa Hospital, Friday, April 10th, 2020 (Period April 5th-8th, 2020)Document4 pagesSyekh Yusuf Gowa Hospital, Friday, April 10th, 2020 (Period April 5th-8th, 2020)DwickyNo ratings yet
- Planned ParenthoodDocument34 pagesPlanned Parenthoodvincentsharon80% (5)
- How To Increase Your Breast Milk Supply: 3-Day ChallengeDocument12 pagesHow To Increase Your Breast Milk Supply: 3-Day ChallengemaynarahsNo ratings yet
- Episiotomy: Dr. Fekadu R (MD) November, 2012/19Document11 pagesEpisiotomy: Dr. Fekadu R (MD) November, 2012/19tareNo ratings yet
- Dialog Present Continous TenseDocument2 pagesDialog Present Continous TenseMessy100% (1)