You might also like
- bb2 Chap7Document12 pagesbb2 Chap7NurRahmaMusdalifaNo ratings yet
- Soft Tissue Tumors: A Practical and Comprehensive Guide to Sarcomas and Benign NeoplasmsFrom EverandSoft Tissue Tumors: A Practical and Comprehensive Guide to Sarcomas and Benign NeoplasmsNo ratings yet
- URO 3 - Neoplasm in The Genitourinary TractDocument8 pagesURO 3 - Neoplasm in The Genitourinary TractHa Jae kyeongNo ratings yet
- Lungs Benign and MalignantDocument7 pagesLungs Benign and MalignantNestley TiongsonNo ratings yet
- L O C S F: IP ND RAL Avity Taging ORMDocument4 pagesL O C S F: IP ND RAL Avity Taging ORMalysonNo ratings yet
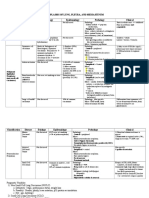
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
- Chapter 11Document10 pagesChapter 11sybico.xray.abadclinicNo ratings yet
- Pathology and Prognostic Determinants of Colorectal Cancer - UpToDateDocument1 pagePathology and Prognostic Determinants of Colorectal Cancer - UpToDateamanuelNo ratings yet
- Salivary Gland TumorsDocument16 pagesSalivary Gland Tumorsmaria del mar RoblesNo ratings yet
- Carcinoma of The LungDocument50 pagesCarcinoma of The LungTristen TanNo ratings yet
- Lung Ca Small Bx2 PDFDocument4 pagesLung Ca Small Bx2 PDFJose SirittNo ratings yet
- 13 AppendixDocument3 pages13 AppendixGibi SupitNo ratings yet
- Nose and Paranasal Sinus Tumours: United Kingdom National Multidisciplinary GuidelinesDocument8 pagesNose and Paranasal Sinus Tumours: United Kingdom National Multidisciplinary GuidelinesRidho RifhansyahNo ratings yet
- EENTDocument11 pagesEENTJohn Christopher LucesNo ratings yet
- TNM Ca de MamaDocument4 pagesTNM Ca de MamaacademiaNo ratings yet
- Urinary Bladder PathologyDocument16 pagesUrinary Bladder Pathologyv@r0_5No ratings yet
- Recto y Ano TraducidoDocument19 pagesRecto y Ano TraducidoJacqueline GómezNo ratings yet
- Chapter 4 - NasopharynxDocument13 pagesChapter 4 - Nasopharynxmaaddy001No ratings yet
- TracheaDocument90 pagesTracheaLpsuedjNo ratings yet
- Testicular Cancer: Basic InformationDocument3 pagesTesticular Cancer: Basic InformationAnonymous eF8cmVvJaNo ratings yet
- TNM - Classifications (1) : 1) UICC-TNM-classification of NETS According To Different Primary TumorsDocument2 pagesTNM - Classifications (1) : 1) UICC-TNM-classification of NETS According To Different Primary TumorsRiaNo ratings yet
- Patologi Tumor Sistim UrogenitalDocument29 pagesPatologi Tumor Sistim UrogenitalSiddiq Blackhell CakepNo ratings yet
- RCJ Finals - Non Epithelial Ovarian CaDocument4 pagesRCJ Finals - Non Epithelial Ovarian CaJohn Paulo Catacutan100% (1)
- Calarynx 130814125710 Phpapp01Document33 pagesCalarynx 130814125710 Phpapp01Wael ShamyNo ratings yet
- Breast Cancer UG Lecture 1Document60 pagesBreast Cancer UG Lecture 1Ribhav GuptaNo ratings yet
- Rect 2Document28 pagesRect 2Miruna GhigeanuNo ratings yet
- " Chest:: by Definition Malignant Tumor of The Lung Primary Its EtiologyDocument10 pages" Chest:: by Definition Malignant Tumor of The Lung Primary Its EtiologyAhmed GaberNo ratings yet
- Soft Tissue SarcomasDocument79 pagesSoft Tissue Sarcomasvinitha kattaNo ratings yet
- Thyroid Malignancy With MRNDDocument25 pagesThyroid Malignancy With MRNDRashma JosephNo ratings yet
- Lung Cancer: I Gede Ketut SajinadiyasaDocument81 pagesLung Cancer: I Gede Ketut Sajinadiyasadr.Dewi Shintaher100% (1)
- 27 Mediastinal and Other Neoplasms Part 2 Other Lung NeoplasmsDocument25 pages27 Mediastinal and Other Neoplasms Part 2 Other Lung NeoplasmsjimmyneumologiaNo ratings yet
- Tumor Laring DannyDocument31 pagesTumor Laring DannyCicha Aulia WardaniNo ratings yet
- SARCOMA Bimbingan KoasDocument41 pagesSARCOMA Bimbingan KoasWarung MamakNo ratings yet
- Female GUDocument18 pagesFemale GULauren LaMonicaNo ratings yet
- DR Sagar Rathod Drddwagh: Presented by GuideDocument1 pageDR Sagar Rathod Drddwagh: Presented by GuideSagarRathodNo ratings yet
- 298658Document44 pages298658Rohan GargNo ratings yet
- Management of Rhabdomyosarco MA: Presenter: DR Manas Dubey Moderator: DR Rakesh DhankharDocument64 pagesManagement of Rhabdomyosarco MA: Presenter: DR Manas Dubey Moderator: DR Rakesh DhankharRebuma MegersaNo ratings yet
- 3-3-08 KnudsonDocument27 pages3-3-08 KnudsonNurRahmaMusdalifaNo ratings yet
- MediastinumDocument38 pagesMediastinumAndreea RalucaNo ratings yet
- Askep CA Paru OkDocument70 pagesAskep CA Paru OkLisa KurniaNo ratings yet
- Oncology NursingDocument6 pagesOncology NursingreooooNo ratings yet
- DR 180114164748Document43 pagesDR 180114164748Hasnain ToheedNo ratings yet
- Imaging in Lung Cancer: Mashuri, Dr. SP - Rad., M.KesDocument54 pagesImaging in Lung Cancer: Mashuri, Dr. SP - Rad., M.KesmirzasullivanNo ratings yet
- CarcinomarectumDocument45 pagesCarcinomarectumHuzefa MemonNo ratings yet
- Presented By: Moderator: Dr. Vikas KumarDocument104 pagesPresented By: Moderator: Dr. Vikas KumarWorku KifleNo ratings yet
- CA M1 RVWR HshsDocument5 pagesCA M1 RVWR HshscharmiemabaoNo ratings yet
- Y1.6 Neoplasia - Malignant Tumors 2022 PDFDocument41 pagesY1.6 Neoplasia - Malignant Tumors 2022 PDFlina hossamNo ratings yet
- Tumors of The Testis: S. Vahidi M.DDocument21 pagesTumors of The Testis: S. Vahidi M.DsuciNo ratings yet
- Squamous Cell CarcinomaDocument5 pagesSquamous Cell CarcinomaNuman QureshiNo ratings yet
- 2010 TNM Staging Colorectal CADocument2 pages2010 TNM Staging Colorectal CAbubbrubb20063998No ratings yet
- Ca of The Respiratory System NCM 112 Cell Ab Final TopicsDocument95 pagesCa of The Respiratory System NCM 112 Cell Ab Final TopicsA. Lizette PabloNo ratings yet
- Rectal Cancer StagingDocument10 pagesRectal Cancer StagingI G. A. Ratna DewiNo ratings yet
- Oleh: DR - Hans Marpaung, SPB, FicsDocument75 pagesOleh: DR - Hans Marpaung, SPB, FicsIrma Julyanti PanggabeanNo ratings yet
- Carcinoma Rectum - Janak - NEWDocument74 pagesCarcinoma Rectum - Janak - NEWTowhidulIslamNo ratings yet
- Case ReportDocument8 pagesCase ReportPradhana FwNo ratings yet
- Family HistoryDocument24 pagesFamily HistoryMARY CLAIRE SUMILHIGNo ratings yet
- Staging Dan Tatalaksana CRDocument13 pagesStaging Dan Tatalaksana CRAyu AnggrainiNo ratings yet
- General Stages and TX of Malignant Cells? Naming TumorsDocument11 pagesGeneral Stages and TX of Malignant Cells? Naming TumorsRyan TurnerNo ratings yet
- Arellano University Senior High School DepartmentDocument3 pagesArellano University Senior High School DepartmentMia QuimsonNo ratings yet
- Disorders of Sexual DevelopmentDocument19 pagesDisorders of Sexual DevelopmentJoanne May100% (1)
- Acne VulgarisDocument58 pagesAcne VulgarisNargisNo ratings yet
- Pharmacology For Nurses A Pathophysiologic Approach 5th Edition Adams Test Bank 1Document34 pagesPharmacology For Nurses A Pathophysiologic Approach 5th Edition Adams Test Bank 1matthew100% (51)
- Support Individuals With Specific Communication NeedsDocument21 pagesSupport Individuals With Specific Communication NeedsRamona Lazurca100% (2)
- MDS Prosthodontics New CurriculumDocument54 pagesMDS Prosthodontics New CurriculumPriyanka GandhiNo ratings yet
- Obesity Research PaperDocument10 pagesObesity Research PaperPaige-Hill88% (16)
- 6 ParoDocument9 pages6 ParoDiana TanasaNo ratings yet
- Full Download Ebook PDF How Writing Works A Guide To Composing Genres PDFDocument41 pagesFull Download Ebook PDF How Writing Works A Guide To Composing Genres PDFpaul.medford293100% (41)
- 5.a. Health Is Wealth LectureDocument62 pages5.a. Health Is Wealth LectureYüshîa Rivás GōmëźNo ratings yet
- Etiopathogenesis and Natural History of Carcinoma Cervix: Human Papilloma Virus High Risk FactorsDocument33 pagesEtiopathogenesis and Natural History of Carcinoma Cervix: Human Papilloma Virus High Risk FactorsNatasya Ayusandra MahersaputriNo ratings yet
- A Project Report ON ''Stress Management'' IN: Master of Business Administration (SESSION 2016-2017)Document73 pagesA Project Report ON ''Stress Management'' IN: Master of Business Administration (SESSION 2016-2017)Sao PutNo ratings yet
- Rekam MedikDocument4 pagesRekam MedikRusmin NoryadinNo ratings yet
- Chapter 84 - Insomnia - Restless Nights and The Blue Moon Level IIDocument6 pagesChapter 84 - Insomnia - Restless Nights and The Blue Moon Level IIaleksme88No ratings yet
- Material Safety Data Sheet Organic Virgin Coconut OilDocument4 pagesMaterial Safety Data Sheet Organic Virgin Coconut OilIda Nur AiniNo ratings yet
- Peperiksaan Pertengahan Tahun 1/2021 Tingkatan 1: SMK Bukit Bandaraya Lorong Maarof, Bangsar, 59000 Kuala LumpurDocument10 pagesPeperiksaan Pertengahan Tahun 1/2021 Tingkatan 1: SMK Bukit Bandaraya Lorong Maarof, Bangsar, 59000 Kuala LumpurjayaselanNo ratings yet
- BRAP PAMET Biosafety Guidance On COVID 19 Testing For Laboratorians EDocument179 pagesBRAP PAMET Biosafety Guidance On COVID 19 Testing For Laboratorians EMM ReyesNo ratings yet
- Case 2 Acute Ischemic Stroke wk.6Document3 pagesCase 2 Acute Ischemic Stroke wk.6Nader AbdurasadNo ratings yet
- Clinical DeathDocument2 pagesClinical DeathIoNo ratings yet
- Emergency First Aid Made Easy Training PresentationDocument92 pagesEmergency First Aid Made Easy Training PresentationRyan-Jay AbolenciaNo ratings yet
- Risk For InfectionDocument5 pagesRisk For InfectionRochelle Corneta JoreNo ratings yet
- ACTIVITY 3: Lifestyle Self-AssessmentDocument5 pagesACTIVITY 3: Lifestyle Self-AssessmentJohn Lloyd SuizoNo ratings yet
- Swanson 2012Document6 pagesSwanson 2012Ramjan KhandelwalNo ratings yet
- Hancock County Needs Assessment 1Document20 pagesHancock County Needs Assessment 1api-622005669No ratings yet
- Previous Gate Questions: Reading ComprehensionDocument17 pagesPrevious Gate Questions: Reading Comprehensionअभिषेक सिंह पटेलNo ratings yet
- Covid 19 Letter To AwaremedDocument2 pagesCovid 19 Letter To AwaremedWMBF NewsNo ratings yet
- Long Covid in PediatricsDocument25 pagesLong Covid in PediatricsAC Vallester100% (1)
- Case 1 Block NBSSDocument13 pagesCase 1 Block NBSSRuswinata ApitoNo ratings yet
- 2 Bedside Case Discussion Evaluation SheetDocument1 page2 Bedside Case Discussion Evaluation Sheetمهند الرحيليNo ratings yet
- Material On Language and Disability PDFDocument25 pagesMaterial On Language and Disability PDFpriyankaNo ratings yet