You might also like
- Antibiotic Dosing Challenges in CKDDocument11 pagesAntibiotic Dosing Challenges in CKDChiranjib BagchiNo ratings yet
- Evaluation Dose of AntibioticDocument3 pagesEvaluation Dose of AntibioticrachmafitriNo ratings yet
- Renal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysFrom EverandRenal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysNo ratings yet
- Effects of Platinum Compounds Viz Cisplatin, Carboplatin & Oxaliplatin On Renal Parameters: A Comparative StudyDocument11 pagesEffects of Platinum Compounds Viz Cisplatin, Carboplatin & Oxaliplatin On Renal Parameters: A Comparative Study9460106212No ratings yet
- Review: Platinum Neurotoxicity PharmacogeneticsDocument8 pagesReview: Platinum Neurotoxicity PharmacogeneticsAndreea TudurachiNo ratings yet
- Renal Dosing of Antibiotics Are We Jumping The GunDocument7 pagesRenal Dosing of Antibiotics Are We Jumping The GunAnaNo ratings yet
- Anticancer Dose Adjustment For Patients With Renal and Hepatic Dysfunction: From Scientific Evidence To Clinical ApplicationDocument16 pagesAnticancer Dose Adjustment For Patients With Renal and Hepatic Dysfunction: From Scientific Evidence To Clinical ApplicationRiz Qie NaNo ratings yet
- Phase II Trial of Curcumin in Patients With Advanced Pancreatic Cancer.Document10 pagesPhase II Trial of Curcumin in Patients With Advanced Pancreatic Cancer.João FrancoNo ratings yet
- How To Adjust Drug Doses in Chronic Kidney DiseaseDocument5 pagesHow To Adjust Drug Doses in Chronic Kidney DiseaseJesse Helmut Hansen-BartelNo ratings yet
- Adverse Events Associated With ERCP: GuidelineDocument16 pagesAdverse Events Associated With ERCP: GuidelineLourdes MarquezNo ratings yet
- 00014Document9 pages00014Gardênia GurgelNo ratings yet
- Journal From Stevens 2009Document3 pagesJournal From Stevens 2009Kezia AngelinaNo ratings yet
- Asia-Pac J CLNCL Oncology - 2023 - Bonazzi - C Reactive Protein Is A Prognostic Biomarker in Pancreatic DuctalDocument10 pagesAsia-Pac J CLNCL Oncology - 2023 - Bonazzi - C Reactive Protein Is A Prognostic Biomarker in Pancreatic DuctalHamsa veniNo ratings yet
- Pancreatic Cancer Literature ReviewDocument10 pagesPancreatic Cancer Literature Reviewea813c29No ratings yet
- Adverse Events ErcpDocument16 pagesAdverse Events ErcpEldaa Prisca Refianti SutantoNo ratings yet
- Chinkenl 2014 PHDDocument227 pagesChinkenl 2014 PHDJesse Helmut Hansen-BartelNo ratings yet
- Palliative Chemotherapy For Advanced Colorectal Cancer Systemati 2000Document5 pagesPalliative Chemotherapy For Advanced Colorectal Cancer Systemati 2000Wiro SablengNo ratings yet
- Prevention of Contrast-Induced Nephropathy (CIN) in Interventional Radiology PracticeDocument12 pagesPrevention of Contrast-Induced Nephropathy (CIN) in Interventional Radiology PracticeReioctabianoNo ratings yet
- Augmented Renal Clearance and How To AugmentDocument12 pagesAugmented Renal Clearance and How To Augmentlocal5.fsgNo ratings yet
- CA Anorexia y Caquexia en OncologiaDocument5 pagesCA Anorexia y Caquexia en OncologiaDiego Bedón AscurraNo ratings yet
- Association Between Statin Use and The Prognosis of Hepatocell - 2023 - EclinicaDocument11 pagesAssociation Between Statin Use and The Prognosis of Hepatocell - 2023 - Eclinicaronaldquezada038No ratings yet
- 8ED94d01 PDFDocument6 pages8ED94d01 PDFIlvita MayasariNo ratings yet
- Wenzel 2005Document8 pagesWenzel 2005cikox21848No ratings yet
- Dosing of Gentamicin in Patients With End-Stage Renal Disease Receiving HemodialysisDocument10 pagesDosing of Gentamicin in Patients With End-Stage Renal Disease Receiving HemodialysisLuciana OliveiraNo ratings yet
- A Study To Assess The Impact of Pharmaceutical Care Services To Cancer Patients in A Tertiary Care HospitalDocument10 pagesA Study To Assess The Impact of Pharmaceutical Care Services To Cancer Patients in A Tertiary Care HospitalRaya PambudhiNo ratings yet
- Measuring Ovarian Toxicity in Clinical Trials AnDocument9 pagesMeasuring Ovarian Toxicity in Clinical Trials AnEdgar LNo ratings yet
- Natural Products For The Management of Castration-Resistant Prostate Cancer: Special Focus On Nanoparticles Based StudiesDocument15 pagesNatural Products For The Management of Castration-Resistant Prostate Cancer: Special Focus On Nanoparticles Based StudiesRajat GoyalNo ratings yet
- Beaumont 2011 Patient Reported Outcomes in Phase III Study of Everolimus Vs PlaceboDocument11 pagesBeaumont 2011 Patient Reported Outcomes in Phase III Study of Everolimus Vs PlaceboIzaty HamidNo ratings yet
- When To Discontinue Renal Replacement TherapyDocument7 pagesWhen To Discontinue Renal Replacement Therapyvali.levo7No ratings yet
- Creatinina2 PDFDocument14 pagesCreatinina2 PDFAngelNo ratings yet
- Barsanti-Innes The Oncologist - 2016Document8 pagesBarsanti-Innes The Oncologist - 2016Liz BethNo ratings yet
- 2012 Best Parctice Medical O Grady TH en FHADocument7 pages2012 Best Parctice Medical O Grady TH en FHASol Del Mar SarmientoNo ratings yet
- Antiemetic Guideline Consistency and Incidence of Chemotherapy-Induced Nausea and Vomiting in US Community Oncology Practice: INSPIRE StudyDocument10 pagesAntiemetic Guideline Consistency and Incidence of Chemotherapy-Induced Nausea and Vomiting in US Community Oncology Practice: INSPIRE StudyKurnia AnharNo ratings yet
- 2021 Molecular Basis of Prostate Cancer. FixDocument40 pages2021 Molecular Basis of Prostate Cancer. FixIrfandi AmiruddinNo ratings yet
- Baseline Blood Work Before Initiation of ChemotherDocument5 pagesBaseline Blood Work Before Initiation of ChemotherChon ChiNo ratings yet
- 1.a Pancreatic CancerDocument8 pages1.a Pancreatic CancerMayracpp.16No ratings yet
- CANT3 Onco-Nephrology - Core Curriculum 2015Document15 pagesCANT3 Onco-Nephrology - Core Curriculum 2015alam25No ratings yet
- 2017 Article 591Document7 pages2017 Article 591Denisse Tinajero SánchezNo ratings yet
- The Search For Disease-Modifying Agents in Decompensated Cirrhosis: From Drug Repurposing To Drug DiscoveryDocument17 pagesThe Search For Disease-Modifying Agents in Decompensated Cirrhosis: From Drug Repurposing To Drug Discoverymuhamad deniansyahNo ratings yet
- First-Line Treatment of Metastatic Renal Cell Carcinoma: A Systematic Review and Network Meta-AnalysisDocument8 pagesFirst-Line Treatment of Metastatic Renal Cell Carcinoma: A Systematic Review and Network Meta-AnalysisDr. Alexandre SatoNo ratings yet
- Hemdan 2014Document6 pagesHemdan 2014DavorIvanićNo ratings yet
- Ca Próstata & Dieta 2020 ZunigaDocument24 pagesCa Próstata & Dieta 2020 ZunigaLuis C Ribon VNo ratings yet
- Clinical-Liver, Pancreas, and Biliary TractDocument8 pagesClinical-Liver, Pancreas, and Biliary TractKirsten HartmanNo ratings yet
- DNA Aptamer Evolved by Cell-SELEX For Recognition ofDocument10 pagesDNA Aptamer Evolved by Cell-SELEX For Recognition ofFernanda LDNo ratings yet
- Desktop IiiDocument9 pagesDesktop IiihenryNo ratings yet
- 9 ErDocument13 pages9 Ermartin Ignacio Zapata LaguadoNo ratings yet
- Ajuste de Dose Dos Medicamentos de Acordo Com A FuDocument7 pagesAjuste de Dose Dos Medicamentos de Acordo Com A FuGraciela CarlosNo ratings yet
- Estimating Renal Function For Drug Dosing Decisions: Mini-ReviewDocument8 pagesEstimating Renal Function For Drug Dosing Decisions: Mini-ReviewnegarayeniNo ratings yet
- Kendzierski 2018Document4 pagesKendzierski 2018Andreas RonaldNo ratings yet
- Clinical Utility of MRCP in Biliary Disease.2653Document2 pagesClinical Utility of MRCP in Biliary Disease.2653Ilham BelgaNo ratings yet
- Baek Et Al. - 2021 - Effect of Mistletoe Extract On Tumor Response in Neoadjuvant Chemoradiotherapy For Rectal Cancer A Cohort StudyDocument10 pagesBaek Et Al. - 2021 - Effect of Mistletoe Extract On Tumor Response in Neoadjuvant Chemoradiotherapy For Rectal Cancer A Cohort StudyMaría Reynel TarazonaNo ratings yet
- CLRRTDocument15 pagesCLRRTArturo ArturoNo ratings yet
- Precision Medicine in Pediatric Oncology: ReviewDocument8 pagesPrecision Medicine in Pediatric Oncology: ReviewCiocan AlexandraNo ratings yet
- Po 22 00246Document10 pagesPo 22 00246ananda febriani auliaNo ratings yet
- Precision Medicine For RheumatologistsDocument9 pagesPrecision Medicine For Rheumatologistsmihaelaatanasova123No ratings yet
- Grothey, Metasadyuvantagosto07Document4 pagesGrothey, Metasadyuvantagosto07Francisco BetancourtNo ratings yet
- HP Mar03 ChronicDocument6 pagesHP Mar03 ChronicAnonymous MJkYnuNo ratings yet
- Pen TingDocument15 pagesPen TingrftdlsNo ratings yet
- 013 - Surgeon-Led-Clinical-Trials-in-Pancrea - 2023 - Surgical-Oncology-Clinics-of-NorDocument9 pages013 - Surgeon-Led-Clinical-Trials-in-Pancrea - 2023 - Surgical-Oncology-Clinics-of-NorDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- SaudiJKidneyDisTranspl321111-4468392 122443Document7 pagesSaudiJKidneyDisTranspl321111-4468392 122443Shakila MaharaniNo ratings yet
- Comparative Treatment Planning Study of Photons and ProtonsDocument15 pagesComparative Treatment Planning Study of Photons and ProtonsJesse Helmut Hansen-BartelNo ratings yet
- Pediatric Nasopharyngeal Carcinoma Treated With Proton Beam Therapy Two Case ReportsDocument5 pagesPediatric Nasopharyngeal Carcinoma Treated With Proton Beam Therapy Two Case ReportsJesse Helmut Hansen-BartelNo ratings yet
- Paediatric Trauma - DR Nicole WilliamsDocument36 pagesPaediatric Trauma - DR Nicole WilliamsJesse Helmut Hansen-BartelNo ratings yet
- Results of Proton ReirradiationDocument9 pagesResults of Proton ReirradiationJesse Helmut Hansen-BartelNo ratings yet
- Facta About Pediatric-Nasopharyngeal-CarcinomaDocument8 pagesFacta About Pediatric-Nasopharyngeal-CarcinomaJesse Helmut Hansen-BartelNo ratings yet
- SVC SyndromeDocument17 pagesSVC SyndromeJesse Helmut Hansen-BartelNo ratings yet
- JZareh Coarctation Aorta Case PresDocument13 pagesJZareh Coarctation Aorta Case PresJesse Helmut Hansen-BartelNo ratings yet
- AinsworthDocument9 pagesAinsworthJesse Helmut Hansen-BartelNo ratings yet
- Filamin A Mutations: Jesse Hansen-BartelDocument8 pagesFilamin A Mutations: Jesse Hansen-BartelJesse Helmut Hansen-BartelNo ratings yet
- Gestational Alloimmune Liver Disease: Ethan TangDocument14 pagesGestational Alloimmune Liver Disease: Ethan TangJesse Helmut Hansen-BartelNo ratings yet
- Study 1Document9 pagesStudy 1Jesse Helmut Hansen-BartelNo ratings yet
- Update in Inflammatory Bowel Disease: Graham MorrisonDocument6 pagesUpdate in Inflammatory Bowel Disease: Graham MorrisonJesse Helmut Hansen-BartelNo ratings yet
- Mar FansDocument14 pagesMar FansJesse Helmut Hansen-BartelNo ratings yet
- Validity of Prediction Models: When Is A Model Clinically Useful?Document20 pagesValidity of Prediction Models: When Is A Model Clinically Useful?Jesse Helmut Hansen-BartelNo ratings yet
- Carboplatin Dosing 2nd Draft DrLinkDocument4 pagesCarboplatin Dosing 2nd Draft DrLinkJesse Helmut Hansen-BartelNo ratings yet
- Study 4Document10 pagesStudy 4Jesse Helmut Hansen-BartelNo ratings yet
- Should We Continue To Use The Cockcroft-Gault Formula?: MinireviewDocument15 pagesShould We Continue To Use The Cockcroft-Gault Formula?: MinireviewJesse Helmut Hansen-BartelNo ratings yet
- Prospective Evaluation of Carboplatin AUC Dosing in Patients With A BMI 27 or CachexiaDocument8 pagesProspective Evaluation of Carboplatin AUC Dosing in Patients With A BMI 27 or CachexiaJesse Helmut Hansen-BartelNo ratings yet
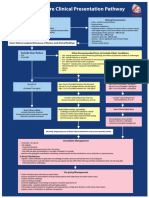
- Heart Failure Clinical Presentation PathwayDocument1 pageHeart Failure Clinical Presentation PathwayJesse Helmut Hansen-BartelNo ratings yet
- Chinkenl 2014 PHDDocument227 pagesChinkenl 2014 PHDJesse Helmut Hansen-BartelNo ratings yet
- Ekhart2009 Article CarboplatinDosingInOverweightADocument8 pagesEkhart2009 Article CarboplatinDosingInOverweightAJesse Helmut Hansen-Bartel100% (1)
- Study 3Document12 pagesStudy 3Jesse Helmut Hansen-BartelNo ratings yet
- Bsa 2Document4 pagesBsa 2Jesse Helmut Hansen-BartelNo ratings yet
- Overestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementDocument7 pagesOverestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementJesse Helmut Hansen-BartelNo ratings yet
- How To Adjust Drug Doses in Chronic Kidney DiseaseDocument5 pagesHow To Adjust Drug Doses in Chronic Kidney DiseaseJesse Helmut Hansen-BartelNo ratings yet
- PublicatiiDocument2 pagesPublicatiiAssani AlexNo ratings yet
- MOH Exam Paper C PDFDocument7 pagesMOH Exam Paper C PDFmidhun0% (1)
- ObsGyn OSCE NotesDocument52 pagesObsGyn OSCE Notesmysorewala100% (11)
- Novi Modusi LečenjaDocument32 pagesNovi Modusi LečenjaDivna CvetkovićNo ratings yet
- Breslow. English Name. 2016Document2 pagesBreslow. English Name. 2016Anca-Raluca PascuNo ratings yet
- PBL Modul 1 Batuk RespiDocument66 pagesPBL Modul 1 Batuk RespiAndiMuhYasserNo ratings yet
- Clinical Atlas of Canine and Feline Dermatology - 2019 - Coyner - IndexDocument12 pagesClinical Atlas of Canine and Feline Dermatology - 2019 - Coyner - Indexnabal22No ratings yet
- Achalasia: A Review of Etiology, Pathophysiology, and TreatmentDocument6 pagesAchalasia: A Review of Etiology, Pathophysiology, and TreatmentAprita NurkarimaNo ratings yet
- Glomerular Diseases: Assistant Professor Dr. Shumaila Rafi MedicineDocument17 pagesGlomerular Diseases: Assistant Professor Dr. Shumaila Rafi MedicineMuhammad MakkiNo ratings yet
- CT Brain Perfusion in The Acute Stroke Setting Maria ScottiDocument52 pagesCT Brain Perfusion in The Acute Stroke Setting Maria ScottiDedi Sutia100% (1)
- Research DesignDocument24 pagesResearch DesignNeza MAe Bulat-ag SalutanNo ratings yet
- Cold Agglutinin DiseaseDocument8 pagesCold Agglutinin Diseasehtunnm@gmail.comNo ratings yet
- Common ICD10 Codes For Acupuncture-1Document1 pageCommon ICD10 Codes For Acupuncture-1Edwin Alvarez100% (1)
- Gestational DiabetesDocument37 pagesGestational DiabetesSathish Kumar ANo ratings yet
- Skippers United Pacific, Inc. vs. Lagne DigestDocument4 pagesSkippers United Pacific, Inc. vs. Lagne DigestEmir MendozaNo ratings yet
- CA Oral CavityDocument53 pagesCA Oral Cavityaakash11No ratings yet
- University College London Medical School (Ucl) : 2-Year Academic Foundation Programmes atDocument16 pagesUniversity College London Medical School (Ucl) : 2-Year Academic Foundation Programmes atPaul CarterNo ratings yet
- Understanding of Usage of Painkillers in The Management of Terminal Cancer PatientDocument6 pagesUnderstanding of Usage of Painkillers in The Management of Terminal Cancer PatientGunners CoolNo ratings yet
- Annotated Answers To Gordis, Epidemiology, 4th Edition QuestionsDocument3 pagesAnnotated Answers To Gordis, Epidemiology, 4th Edition Questionssdverde100% (1)
- Cultivating Qi Healer PDFDocument7 pagesCultivating Qi Healer PDFAlina TudoracheNo ratings yet
- Hemorrhoids: What Are Hemorroids?Document2 pagesHemorrhoids: What Are Hemorroids?Igor DemićNo ratings yet
- Linfedema en Mexico: Un Panorama Clínico y EpidemiologicoDocument11 pagesLinfedema en Mexico: Un Panorama Clínico y EpidemiologicoEnrique LopezNo ratings yet
- Chemistry ProjectDocument17 pagesChemistry ProjectSurajNo ratings yet
- Diabetic Microvascular DiseaseDocument68 pagesDiabetic Microvascular DiseasePavel GonzálezNo ratings yet
- NH4OH MsdsDocument6 pagesNH4OH MsdsZoelFikar FahmiNo ratings yet
- Developmental Anamolies of Soft Tissues of Oral CavityDocument73 pagesDevelopmental Anamolies of Soft Tissues of Oral Cavityvellingiriramesh53040% (1)
- Glomerular DiseaseDocument98 pagesGlomerular DiseasePatrick TumewuNo ratings yet
- Dermatitis Atopik PDFDocument11 pagesDermatitis Atopik PDFmlengseNo ratings yet
- WIMJ2017 Vol 4, Issue 1 Complete PDFDocument76 pagesWIMJ2017 Vol 4, Issue 1 Complete PDFarvind YadavNo ratings yet
- Intermittent Vs Indwelling CatheterizationDocument2 pagesIntermittent Vs Indwelling CatheterizationWildan DzakiyNo ratings yet