You might also like
- Choosing The Best Operation For Chronic Subdural Hematoma - A Decision Analysis (Journal of Neurosurgery)Document7 pagesChoosing The Best Operation For Chronic Subdural Hematoma - A Decision Analysis (Journal of Neurosurgery)Mon ChávezNo ratings yet
- Outcome Analysis and Prognostic Factors in Patients of Glioblastoma Multiforme An Indonesian Single Institution ExperienceDocument7 pagesOutcome Analysis and Prognostic Factors in Patients of Glioblastoma Multiforme An Indonesian Single Institution Experienceafdhal.888980No ratings yet
- Brain Cancer Progression A Retrospective.7Document9 pagesBrain Cancer Progression A Retrospective.7Hamzeh AlsalhiNo ratings yet
- Neurología: Traumatic Brain Injury in The New Millennium: New Population and New ManagementDocument7 pagesNeurología: Traumatic Brain Injury in The New Millennium: New Population and New Managementja.arenas904pfizerNo ratings yet
- Surgical Neurology International: Chronic Subdural Hematoma: Surgical Management and OutcomeDocument9 pagesSurgical Neurology International: Chronic Subdural Hematoma: Surgical Management and OutcomeSelfa YunitaNo ratings yet
- Craniopharyngioma 2 PDFDocument9 pagesCraniopharyngioma 2 PDFBea NufuarNo ratings yet
- 793 FullDocument9 pages793 FullDENNYNo ratings yet
- 2019 Damico PROs and PROMs in MSDocument6 pages2019 Damico PROs and PROMs in MSMaría Pía BalmacedaNo ratings yet
- Pediatric JournalDocument11 pagesPediatric JournalHenny WijayaNo ratings yet
- MD 92 285Document9 pagesMD 92 285Pulmonologi Dan Kedokteran Respirasi FK UNRINo ratings yet
- Bacterial Brain Abscess: An Outline For Diagnosis and ManagementDocument10 pagesBacterial Brain Abscess: An Outline For Diagnosis and ManagementWIWI HRNo ratings yet
- Factors Influencing The Outcome of Patients With Acute Extradural Haematomas Undergonig SurgeryDocument9 pagesFactors Influencing The Outcome of Patients With Acute Extradural Haematomas Undergonig SurgeryAlexis MutuyimanaNo ratings yet
- nihms271845Document17 pagesnihms271845Andres Mauricio MuñozNo ratings yet
- Int Forum Allergy Rhinol - 2018 - Mattos - Establishing The Minimal Clinically Important Difference For The QuestionnaireDocument6 pagesInt Forum Allergy Rhinol - 2018 - Mattos - Establishing The Minimal Clinically Important Difference For The QuestionnaireSid TNo ratings yet
- [19330693 - Journal of Neurosurgery] Patient factors associated with 30-day morbidity, mortality, and length of stay after surgery for subdural hematoma_ a study of the American College of Surgeons National SurgiDocument7 pages[19330693 - Journal of Neurosurgery] Patient factors associated with 30-day morbidity, mortality, and length of stay after surgery for subdural hematoma_ a study of the American College of Surgeons National SurgiBruno MañonNo ratings yet
- Diagnostic Value of Circulating Tumor DNA in Molecular Characterization of GliomaDocument8 pagesDiagnostic Value of Circulating Tumor DNA in Molecular Characterization of GliomaAnyaNo ratings yet
- A Systematic Review and Meta-Analysis Examining The Impact of Incident Postoperative Delirium On MortalityDocument11 pagesA Systematic Review and Meta-Analysis Examining The Impact of Incident Postoperative Delirium On MortalitypablopabloortizortizNo ratings yet
- KJN 12 47Document8 pagesKJN 12 47Khenza Nur HasanahNo ratings yet
- Car Gade Delirium e Nuc IDocument20 pagesCar Gade Delirium e Nuc INataly Audrey Romero DiazNo ratings yet
- Factors For Second Non-Diagnostic Ultrasound-Guided Fine-Needle Aspiration Cytology in Thyroid NodulesDocument10 pagesFactors For Second Non-Diagnostic Ultrasound-Guided Fine-Needle Aspiration Cytology in Thyroid Nodulesmiguel saba sabaNo ratings yet
- Alteraciones Adultos MayoresDocument12 pagesAlteraciones Adultos MayoresGabriel Zúñiga MartinezNo ratings yet
- Case Study Intramedullary Spinal Cord TumorDocument13 pagesCase Study Intramedullary Spinal Cord TumorCitra KristiNo ratings yet
- Traumatic Brain Injury in Children Under Age 24 Months: Analysis of Demographic Data, Risk Factors, and Out-Comes of Post-Traumatic SeizureDocument7 pagesTraumatic Brain Injury in Children Under Age 24 Months: Analysis of Demographic Data, Risk Factors, and Out-Comes of Post-Traumatic SeizureSanti NurfitrianiNo ratings yet
- Safety of Middle Meningeal Artery Embolization For Treatment of Subdural Hematoma - A Nationwide Propensity Score Matched AnalysisDocument10 pagesSafety of Middle Meningeal Artery Embolization For Treatment of Subdural Hematoma - A Nationwide Propensity Score Matched AnalysisJUANNo ratings yet
- Cancers 14 03161Document10 pagesCancers 14 03161Majd AssaadNo ratings yet
- Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in The US From December 2020 To August 2021Document10 pagesMyocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in The US From December 2020 To August 2021Jim Hoft100% (3)
- Fisioterapia Hematoma SubduralDocument4 pagesFisioterapia Hematoma SubduralLeandro AntivilNo ratings yet
- Fonc 10 01662Document12 pagesFonc 10 01662Bose BabuNo ratings yet
- Ventricular Septal Defect Complicating ST-Elevation Myocardial Infarctions: A Call For ActionDocument12 pagesVentricular Septal Defect Complicating ST-Elevation Myocardial Infarctions: A Call For ActionIde Yudis TiyoNo ratings yet
- HospitalDocument5 pagesHospitalhinatakunhinata75No ratings yet
- Tga Article 2Document9 pagesTga Article 2MYMANo ratings yet
- (Journal of Neurosurgery - Spine) Risk Factors For Deep Surgical Site Infection Following Thoracolumbar Spinal SurgeryDocument10 pages(Journal of Neurosurgery - Spine) Risk Factors For Deep Surgical Site Infection Following Thoracolumbar Spinal SurgeryEugenia BocaNo ratings yet
- Can Progression of Odontogenic Infections To Cervical Necrotizing Soft Tissue InfectionsDocument8 pagesCan Progression of Odontogenic Infections To Cervical Necrotizing Soft Tissue InfectionsFadly RasyidNo ratings yet
- Jamadermatology Kridin 2021 Oi 210045 1634154542.6481Document9 pagesJamadermatology Kridin 2021 Oi 210045 1634154542.6481Nandha KumarNo ratings yet
- 2014 Delirium in Elderly PeopleDocument12 pages2014 Delirium in Elderly Peoplejuan.pablo.castroNo ratings yet
- 1 s2.0 S2352914822000557 MainDocument7 pages1 s2.0 S2352914822000557 MainGracia BarimanNo ratings yet
- Jama Oster 2022 Oi 210145 1647635624.12259Document10 pagesJama Oster 2022 Oi 210145 1647635624.12259Zoltán BaloghNo ratings yet
- The Addition of Paclitaxel To Doxorubicin and Cisplatin and Cispalatin Volume Directed RadiationDocument21 pagesThe Addition of Paclitaxel To Doxorubicin and Cisplatin and Cispalatin Volume Directed RadiationGarsa GarnolNo ratings yet
- Brain Tumor Thesis StatementDocument8 pagesBrain Tumor Thesis Statementchristinamartinspringfield100% (2)
- A Systematic Review of The Drug-Induced - I - I - Stevens-Johnson Syndrome - I - I - and Toxic Epidermal Necrolysis in Indian PopulationDocument10 pagesA Systematic Review of The Drug-Induced - I - I - Stevens-Johnson Syndrome - I - I - and Toxic Epidermal Necrolysis in Indian PopulationMiss AmyNo ratings yet
- Neuroimage: ClinicalDocument16 pagesNeuroimage: ClinicalAniket AmanNo ratings yet
- CTS MHDDocument8 pagesCTS MHDTheodoreNo ratings yet
- NIH Public Access: Author ManuscriptDocument22 pagesNIH Public Access: Author ManuscriptHumberto QuimeNo ratings yet
- 3 Pages Review-Mcdonald2018Document3 pages3 Pages Review-Mcdonald2018Riyan PratamaNo ratings yet
- (10920684 - Neurosurgical Focus) Impact of Preoperative Endovascular Embolization On Immediate Meningioma Resection OutcomesDocument7 pages(10920684 - Neurosurgical Focus) Impact of Preoperative Endovascular Embolization On Immediate Meningioma Resection OutcomesBedussa NuritNo ratings yet
- Prognostic Biomarkers for Survival in Nasopharyngeal Carcinoma - A Systematic Review of the LiteratureDocument14 pagesPrognostic Biomarkers for Survival in Nasopharyngeal Carcinoma - A Systematic Review of the LiteratureWening Dewi HapsariNo ratings yet
- The Oncologist 2003 Weinstein 278 92Document15 pagesThe Oncologist 2003 Weinstein 278 92Josne J. PaezNo ratings yet
- fnagi-15-1184435Document15 pagesfnagi-15-1184435maria fensterseiferNo ratings yet
- Association Between Resilience and Quality of Life in Patients With Colon CancerDocument7 pagesAssociation Between Resilience and Quality of Life in Patients With Colon CancerICR CONSULTORESNo ratings yet
- Han 2017Document4 pagesHan 2017Alexandria Firdaus Al-farisyNo ratings yet
- Provenge 2Document12 pagesProvenge 2api-675909478No ratings yet
- (10920684 - Neurosurgical Focus) Predictors of Outcome of Subdural Empyema in ChildrenDocument6 pages(10920684 - Neurosurgical Focus) Predictors of Outcome of Subdural Empyema in ChildrenFatima RamirezNo ratings yet
- Ournal of Linical Ncology: PurposeDocument8 pagesOurnal of Linical Ncology: PurposerimaNo ratings yet
- Jco 22 02347Document11 pagesJco 22 02347Quang Thái NguyễnNo ratings yet
- Prognostic Significance of Hematologic Markers in Patients With Head and Neck Squamous Cell CarcinomasDocument11 pagesPrognostic Significance of Hematologic Markers in Patients With Head and Neck Squamous Cell CarcinomasLeyla M HattaNo ratings yet
- Yang 2020Document9 pagesYang 2020lucasnegromonte0001No ratings yet
- Esclerosis Tuberosa 6Document18 pagesEsclerosis Tuberosa 6Santiago CeliNo ratings yet
- (10920684 - Neurosurgical Focus) Patterns in Neurosurgical Adverse Events - Intracranial Neoplasm SurgeryDocument9 pages(10920684 - Neurosurgical Focus) Patterns in Neurosurgical Adverse Events - Intracranial Neoplasm SurgeryLusy Octavia SaputriNo ratings yet
- Brain Tumors in ChildrenFrom EverandBrain Tumors in ChildrenAmar GajjarNo ratings yet
- Innovations in Modern Endocrine SurgeryFrom EverandInnovations in Modern Endocrine SurgeryMichael C. SingerNo ratings yet
- Upregulation of Mir-196B Confers A Poor Prognosis in Glioblastoma Patients Via Inducing A Proliferative PhenotypeDocument7 pagesUpregulation of Mir-196B Confers A Poor Prognosis in Glioblastoma Patients Via Inducing A Proliferative PhenotypeALINo ratings yet
- PD-L1 Expression by Neurons Nearby Tumors Indicates Better Prognosis in Glioblastoma PatientsDocument15 pagesPD-L1 Expression by Neurons Nearby Tumors Indicates Better Prognosis in Glioblastoma PatientsALINo ratings yet
- GB 16Document5 pagesGB 16ALINo ratings yet
- Impact of Genotype and Morphology On The Prognosis of GlioblastomaDocument8 pagesImpact of Genotype and Morphology On The Prognosis of GlioblastomaALINo ratings yet
- GB 10Document9 pagesGB 10ALINo ratings yet
- GB 2Document7 pagesGB 2ALINo ratings yet
- Low Serum Level of Mir-485-3P Predicts Poor Survival in Patients With GlioblastomaDocument11 pagesLow Serum Level of Mir-485-3P Predicts Poor Survival in Patients With GlioblastomaALINo ratings yet
- Original Article: High Expression of WDR1 in Primary Glioblastoma Is Associated With Poor PrognosisDocument12 pagesOriginal Article: High Expression of WDR1 in Primary Glioblastoma Is Associated With Poor PrognosisALINo ratings yet
- Prognostic Factors For Long-Term Survival After GlioblastomaDocument4 pagesPrognostic Factors For Long-Term Survival After GlioblastomaALINo ratings yet
- Original Article: High Expression of WDR1 in Primary Glioblastoma Is Associated With Poor PrognosisDocument12 pagesOriginal Article: High Expression of WDR1 in Primary Glioblastoma Is Associated With Poor PrognosisALINo ratings yet
- Predicting Glioblastoma Prognosis Networks Using Weighted Gene Co-Expression Network Analysis On TCGA DataDocument8 pagesPredicting Glioblastoma Prognosis Networks Using Weighted Gene Co-Expression Network Analysis On TCGA DataALINo ratings yet
- Surgical Neurology International: Socioeconomic Status Does Not Affect Prognosis in Patients With Glioblastoma MultiformeDocument9 pagesSurgical Neurology International: Socioeconomic Status Does Not Affect Prognosis in Patients With Glioblastoma MultiformeALINo ratings yet
- The Importance of Genomic Copy Number Changes in The Prognosis of Glioblastoma MultiformeDocument7 pagesThe Importance of Genomic Copy Number Changes in The Prognosis of Glioblastoma MultiformeALINo ratings yet
- Upregulation of Mir-196B Confers A Poor Prognosis in Glioblastoma Patients Via Inducing A Proliferative PhenotypeDocument7 pagesUpregulation of Mir-196B Confers A Poor Prognosis in Glioblastoma Patients Via Inducing A Proliferative PhenotypeALINo ratings yet
- Low Serum Level of Mir-485-3P Predicts Poor Survival in Patients With GlioblastomaDocument11 pagesLow Serum Level of Mir-485-3P Predicts Poor Survival in Patients With GlioblastomaALINo ratings yet
- Predicting Glioblastoma Prognosis Networks Using Weighted Gene Co-Expression Network Analysis On TCGA DataDocument8 pagesPredicting Glioblastoma Prognosis Networks Using Weighted Gene Co-Expression Network Analysis On TCGA DataALINo ratings yet
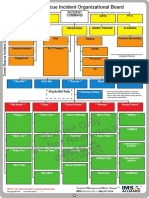
- Sample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardDocument1 pageSample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardLuis Diaz CerdanNo ratings yet
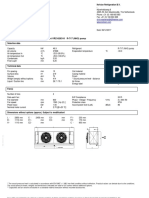
- GSL DIP Phase - 1 Cooler 45kWDocument1 pageGSL DIP Phase - 1 Cooler 45kWMuhasin PallikkalNo ratings yet
- Financing of New EnterpriseDocument8 pagesFinancing of New EnterpriseSunil BhamuNo ratings yet
- Waste Management in Vienna. MA 48Document12 pagesWaste Management in Vienna. MA 484rtttt4ttt44No ratings yet
- MUSCULAR SYSTEM WORKSHEET Slides 1 To 4Document4 pagesMUSCULAR SYSTEM WORKSHEET Slides 1 To 4kwaiyuen ohnNo ratings yet
- Factors to Consider in Reactor Design for Industrial ProcessesDocument3 pagesFactors to Consider in Reactor Design for Industrial Processesuma villashini100% (2)
- 978 613 8 91055 8 PDFDocument309 pages978 613 8 91055 8 PDFEr Sayan ParamanikNo ratings yet
- Design of Temporary Floating Road for Construction SiteDocument6 pagesDesign of Temporary Floating Road for Construction SiteAnonymous hRWwL7pZnCNo ratings yet
- Quest The Last RemnantDocument67 pagesQuest The Last Remnantding suheNo ratings yet
- Engineering Statics FundamentalsDocument28 pagesEngineering Statics FundamentalsurwaNo ratings yet
- Worthy - Elevation WorshipDocument1 pageWorthy - Elevation WorshipSabine J.100% (1)
- Slovakia C1 TestDocument7 pagesSlovakia C1 TestĐăng LêNo ratings yet
- Labcelldivision ErikagutierrezDocument10 pagesLabcelldivision Erikagutierrezapi-336047220No ratings yet
- Bandari 2015 Exact SER Expressions of GFDM in Nakagami-M and Rician Fading ChannelsDocument6 pagesBandari 2015 Exact SER Expressions of GFDM in Nakagami-M and Rician Fading Channelssameer khan100% (1)
- Entrepreneurship Macro Environment ForcesDocument26 pagesEntrepreneurship Macro Environment ForcesSivaNo ratings yet
- Maha VairocanaDocument8 pagesMaha VairocanaDavid Moerler100% (3)
- Rate Analysis-Norms 1Document10 pagesRate Analysis-Norms 1yamanta_rajNo ratings yet
- Entry-Exit Arrangement With Service RoadDocument1 pageEntry-Exit Arrangement With Service RoadRamBhuvan SonkarNo ratings yet
- Fiber Crops - FlaxDocument33 pagesFiber Crops - Flaxmalath bashNo ratings yet
- To Begin: MantraDocument9 pagesTo Begin: MantraashissahooNo ratings yet
- Ceiling Fans Sensa Series: F Yuragi Function (Natural Breeze)Document1 pageCeiling Fans Sensa Series: F Yuragi Function (Natural Breeze)TYNo ratings yet
- Kraby System 2018Document22 pagesKraby System 2018soga010178No ratings yet
- Understanding and Quantifying Mountain TourismDocument84 pagesUnderstanding and Quantifying Mountain TourismfloridNo ratings yet
- 21st Century Science - Summer 2011 - The Universe Is CreativeDocument84 pages21st Century Science - Summer 2011 - The Universe Is CreativeMatthew EhretNo ratings yet
- Path Loss Models and Wireless Propagation EffectsDocument17 pagesPath Loss Models and Wireless Propagation EffectsAhsan RafiqNo ratings yet
- PTC Document Status: (Updated 11 November 2015)Document5 pagesPTC Document Status: (Updated 11 November 2015)AndersonGabriel23No ratings yet
- Catalogo Tecnico Gb-S v07Document29 pagesCatalogo Tecnico Gb-S v07farou9 bmzNo ratings yet
- Foundation of EducationDocument31 pagesFoundation of EducationM T Ząřřąř100% (1)
- Guide 111: International Electrotechnical CommissionDocument7 pagesGuide 111: International Electrotechnical CommissionSayyid JifriNo ratings yet
- Determining The Thickness of Glass in Airport Traffic Control Tower CabsDocument17 pagesDetermining The Thickness of Glass in Airport Traffic Control Tower CabsAdán Cogley CantoNo ratings yet














![[19330693 - Journal of Neurosurgery] Patient factors associated with 30-day morbidity, mortality, and length of stay after surgery for subdural hematoma_ a study of the American College of Surgeons National Surgi](https://imgv2-1-f.scribdassets.com/img/document/722525704/149x198/264ee18e78/1712965540?v=1)