Professional Documents
Culture Documents
Jurnal 7
Uploaded by
Ahmad Fari Arief LopaCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Jurnal 7
Uploaded by
Ahmad Fari Arief LopaCopyright:
Available Formats
Cardiopulmonar y Imaging • Original Research
Chung et al.
CT Findings, Radiologic-Pathologic Correlation, and Predictors
of Survival for Patients With IPAF
Cardiopulmonary Imaging
Original Research
CT Findings, Radiologic-Pathologic
Correlation, and Imaging
Downloaded from www.ajronline.org by 125.167.114.159 on 05/24/21 from IP address 125.167.114.159. Copyright ARRS. For personal use only; all rights reserved
Predictors of Survival for Patients
With Interstitial Pneumonia With
Autoimmune Features
Jonathan H. Chung1 OBJECTIVE. The objective of this study is to determine the CT findings and patterns of
Steven M. Montner 1 interstitial pneumonia with autoimmune features (IPAF) and to assess whether imaging can
Ayodeji Adegunsoye2 predict survival for patients with IPAF.
Cathryn Lee2 MATERIALS AND METHODS. The study included 136 subjects who met the criteria
Justin M. Oldham 3 for IPAF and had diagnostic-quality chest CT scans obtained from 2006 to 2015; a total of 74
of these subjects had pathologic samples available for review within 1 year of chest CT ex-
Aliya N. Husain 4
amination. CT findings and the presence of an usual interstitial pneumonitis (UIP) pattern of
Heber MacMahon1 disease were assessed, as was the UIP pattern noted on pathologic analysis. Analysis of chest
Imre Noth2 CT findings associated with survival was performed using standard univariate and multivari-
Rekha Vij2 ate Cox proportional hazards methods as well as the unadjusted log-rank test. Survival data
Mary E. Strek 2 were visually presented using the Kaplan-Meier survival curve estimator.
RESULTS. Most subjects with IPAF (57.4%; 78/136) had a high-confidence diagnosis of a
Chung JH, Montner SM, Adegunsoye A, et al.
UIP pattern on CT. Substantially fewer subjects (28.7%; 39/136) had a pattern that was incon-
sistent with UIP noted on CT. The presence of a UIP pattern on CT was associated with smok-
ing (p < 0.01), male sex (p < 0.01), and older age (p < 0.001). Approximately one-fourth of the
subjects had a nonspecific interstitial pneumonitis pattern on CT. Of interest, nearly one-tenth
of the subjects had a CT pattern that was most consistent with hypersensitivity pneumonitis
rather than the customary CT patterns ascribed to lung disease resulting from connective tis-
sue disease. Most subjects with a possible UIP pattern on CT (83.3%) had UIP diagnosed on
Keywords: connective tissue disease, CT, interstitial
the basis of pathologic findings. Focused multivariate analysis showed that honeycombing on
pneumonia with autoimmune features, survival, usual CT (hazard ratio, 2.17; 95% CI, 1.05–4.47) and pulmonary artery enlargement on CT (hazard
interstitial pneumonitis ratio, 2.08; 95% CI, 1.02–4.20) were independent predictors of survival.
CONCLUSION. IPAF most often presents with a UIP pattern on CT and is associated with
DOI:10.2214/AJR.16.17121
worse survival when concomitant honeycombing or pulmonary artery enlargement is present.
Received July 21, 2016; accepted after revision
t has been recognized that a sub- [1]. The proposed criteria include traditional
I
October 27, 2016.
1
stantial proportion of patients clinical and serologic features of CTD; mor-
Department of Radiology, University of Chicago
Medical Center, 5841 S Maryland Ave, Chicago, IL
with idiopathic interstitial pneu- phologic features consistent with CTD, as
60637. Address correspondence to J. H. Chung monia (IIP) have signs and determined from the subdomains of chest ra-
(jonherochung@uchicago.edu). symptoms suggestive of an underlying auto- diographic imaging and histopathologic
2
immune process but do not meet the defined analysis; and physiologic features identified
Section of Pulmonary/Critical Care, Department of
criteria for a specific connective tissue dis- from pulmonary function tests.
Medicine, University of Chicago Medical Center,
Chicago, IL. ease (CTD). The differences in interstitial The imaging patterns and prognostic sig-
lung disease (ILD) associated with diag- nificance of the IPAF classification have yet
3
Section of Pulmonary/Critical Care, Department of nosed or suspected CTD, compared with oth- to be fully defined. Previous studies of pa-
Medicine, University of California at Davis, er types of ILD, is an ongoing field of study. tients with disease classifications similar to
Sacramento, CA.
A multisociety task force introduced new re- IPAF (e.g., lung-dominant CTD, undifferenti-
4
Department of Pathology, University of Chicago Medical search criteria for interstitial pneumonia ated CTD [UCTD]–associated ILD, and ILD
Center, Chicago, IL. with autoimmune features (IPAF), in an at- with autoimmune features) have shown differ-
tempt “to derive a uniform name and set of ing results that are likely related to differences
AJR 2017; 208:1229–1236 classification criteria for patients with IIP in the criteria for diagnosis [1–4]. One of the
0361–803X/17/2086–1229
and an autoimmune flavor” separate from pa- goals of the IPAF classification is to develop a
tients with ILD who do not have evidence of consistent platform from which to rigorously
© American Roentgen Ray Society autoimmune components or a defined CTD study this specific group of patients.
AJR:208, June 2017 1229
Chung et al.
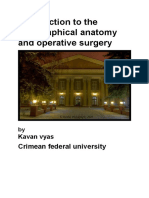
Fig. 1—75-year-old man with
interstitial pneumonia with
autoimmune features.
A and B, Axial (A) and coronal (B)
chest CT images show peripheral
and basilar predominant
distribution of pulmonary fibrosis
Downloaded from www.ajronline.org by 125.167.114.159 on 05/24/21 from IP address 125.167.114.159. Copyright ARRS. For personal use only; all rights reserved
characterized by reticulation,
traction bronchiectasis, traction
bronchiolectasis, and subpleural
honeycombing consistent with
usual interstitial pneumonitis.
A B
The main objective of the present study Materials and Methods ent study, we report the specific CT findings for
is to document in detail the CT features of Subjects and Clinical Information IPAF as well as the CT findings associated with
IPAF, on the basis of a systematic review This retrospective study was HIPAA compli- the survival of patients with IPAF. Oldham and
of a large number of CT scans and corre- ant and was approved by our institutional review colleagues analyzed survival mainly on the basis
sponding patient medical records at our board (number 14163-A). of pathologic findings.
medical center. Given that most patients The ILD research registry at the University of IPAF was diagnosed using the current research
with CTD-associated ILD (with the ex- Chicago Medical Center was used to identify adults guidelines, which comprise clinical, serologic, and
ception of rheumatoid arthritis) have mor- who were evaluated in the ILD clinic from 2006 to morphologic (i.e., imaging, pathologic, and phys-
phologic findings of nonspecific interstitial 2015. Patients with idiopathic pulmonary fibrosis, iologic) features [8]. We obtained clinical data
pneumonia (NSIP), organizing pneumo- unclassifiable IIP, biopsy-proven idiopathic NSIP, from patients at their initial clinic visit, including
nia, or both, and given that many CT find- and biopsy-proven organizing pneumonia were iden- demographic characteristics, history, medication
ings inconsistent with UIP [5] support the tified [5]. Patients who were given an interim diagno- use, physical examination findings, and laborato-
diagnosis of IPAF, we expect that the CT sis of UCTD-associated ILD on the basis of previous ry findings (which included findings from a com-
appearance would most often be inconsis- criteria were also identified [2]. ILD was diagnosed prehensive serologic assessment). Anti–clinically
tent with UIP. The second objective of this using a multidisciplinary approach. Follow-up was amyopathic dermatomyositis-140 (melanoma dif-
study is to assess which, if any, CT find- censored on December 1, 2015. Subjects were ex- ferentiation-associated protein 5) autoantibody and
ings are predictive of survival for patients cluded from the study if they had a known cause of anti–polymyositis/scleroderma antibodies were not
with IPAF. Imaging findings have been ILD, declined to provide informed consent, or did included in the routine evaluation of ILD at our
shown to predict survival in the setting of not undergo the necessary tests (i.e., serologic as- medical center; therefore, they could not be as-
IIP; however, in the setting of CTD, the sig- sessment, chest CT, or surgical lung biopsy) needed sessed. Data from pulmonary function tests were
nificance of imaging findings is less clear, to achieve a confident diagnosis of IPAF. also assessed, including the percentage of predict-
and in IPAF, it is unknown [6]. We hypoth- Of the 1045 patients in the ILD registry, 144 ed forced vital capacity, the percentage of predicted
esize that, similar to idiopathic ILD, the met the criteria for IPAF reported by Oldham et total lung capacity, and the percentage of predicted
presence of a UIP pattern and macroscop- al. [7]. Of these 144 patients, 136 had diagnos- diffusion capacity of the lung for carbon monoxide.
ic CT findings of pulmonary fibrosis (e.g., tic-quality chest CT scans available for review.
honeycombing, reticulation, and traction Oldham and colleagues reported the presenting CT Evaluation
bronchiectasis) would be associated with features of a cohort with IPAF from the clini- The earliest diagnostic-quality chest CT scan
decreased survival. cal pulmonary perspective, whereas in the pres- obtained for each subject was scored. Studies from
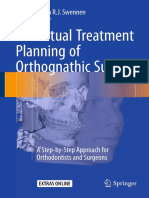
Fig. 2—48-year-old woman
with interstitial pneumonia with
autoimmune features.
A and B, Axial (A) and coronal (B) chest
CT images show peripheral and basilar
predominant distribution of pulmonary
fibrosis characterized by reticulation,
traction bronchiectasis, and traction
bronchiolectasis without subpleural
honeycombing consistent with possible
usual interstitial pneumonitis pattern.
A B
1230 AJR:208, June 2017
CT Findings, Radiologic-Pathologic Correlation, and Predictors of Survival for Patients With IPAF
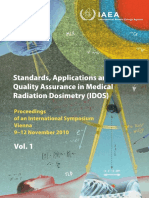
Fig. 3—79-year-old woman
with interstitial pneumonia with
autoimmune features.
A and B, Axial (A) and coronal (B)
CT images show axially diffuse
and upper zone preponderant lung
disease characterized by ground-
Downloaded from www.ajronline.org by 125.167.114.159 on 05/24/21 from IP address 125.167.114.159. Copyright ARRS. For personal use only; all rights reserved
glass opacity and reticulation
diagnostic of pattern inconsistent
with usual interstitial pneumonitis,
given degree of ground-glass opacity
and upper lung preponderance.
A B
outside hospitals were reviewed if their image quality with regard to these categories was scored to the as appropriate. A two-tailed Fisher exact test or
was adequate, resulting in a total of 18 of the 136 CT nearest 5%. Multicompartment involvement [8] chi-square test was used to compare proportions.
evaluated scans originating from outside hospitals. was systematically evaluated on chest CT by as- Mean values for continuous variables between
The criteria for determining whether an image was sessing the presence of pleural effusion or thicken- groups were compared using a two-tailed t (para-
of diagnostic quality included thin-section acquisi- ing, pericardial effusion or thickening, mosaic at- metric) test or a Mann-Whitney U (nonparametric)
tion or reconstruction (< 2.0 mm) through the whole tenuation in the absence of visible emphysema, and test. Analysis of chest CT findings associated with
thorax and absence of significant motion artifact nontraction bronchiectasis, as well as by determin- survival was performed using standard univariate
that obscured the lung parenchymal detail. High- ing the diameter of the pulmonary artery [9]. We and multivariate Cox proportional hazards meth-
resolution CT was performed at our medical center corrected mosaic attenuation for emphysema (as a odology as well as the unadjusted log-rank test.
with the use of various scanners, including 16- and marker of substantial injury to the lungs caused by Survival was visually presented using the Kaplan-
64-MDCT scanners (Brilliance, Philips Healthcare) smoking), given that small airways disease is com- Meier survival curve estimator. Time from diag-
or a 256-MDCT scanner (Brilliance iCT, Philips monly associated with smoking and may have con- nosis to either death or lung transplantation was
Healthcare). Helical CT acquisition was performed founded statistical analyses [10]. A threshold of 3.3 used as the endpoint. The multivariate analysis of
during full inspiration with the patient in the supine cm for pulmonary artery enlargement was used to survival included chest CT variables thought to af-
position, with the use of a tube voltage of 120 kVp, increase the specificity of this finding [11, 12]. fect survival in biologically plausible independent
a tube current-time product of 220 mAs, and image As per guidelines, the level of confidence in a pathways; thus, only honeycombing (as the major
reconstruction with a 512 × 512 pixel image ma- CT diagnosis of IPAF relative to UIP was scored proxy for end-stage fibrosis), mosaic attenuation
trix. Transverse (axial) images were reconstructed as UIP, possible UIP, or inconsistent with UIP [5, (as a proxy for small airways disease), and ground-
contiguously at slice thicknesses of 1.0 mm and 3.0 13–17] (Figs. 1–3). If the pattern noted on CT was glass opacity (as a proxy for pulmonary inflamma-
mm, with the use of a standard lung kernel. Coro- not definitely UIP, the readers also selected by con- tion) were included. The analysis was adjusted for
nal and sagittal images were reconstructed at a slice sensus the best overall alternative imaging-based the GAP (gender, age, and physiology [forced vital
thickness of 2.5 mm. End-expiratory phase helical diagnosis, including the whole spectrum of IIP, capacity and diffused capacity of the lung for car-
CT images were also obtained at a tube voltage of hypersensitivity pneumonitis (HP), sarcoidosis, ob- bon monoxide]) score [18] and the positivity of the
120 kVp, a tube current-time product of 60 mA, and literative bronchiolitis, asbestosis, silicosis, and cel- clinical domain (i.e., clinical, serologic, and mor-
contiguous reconstruction of 3-mm slices, as were lular bronchiolitis, with a level of confidence (i.e., phologic), as defined for IPAF classification [8].
transverse 1-mm images (thickness, 1.2 × 10 mm) possible, probable, or definite). All statistical studies were performed using statis-
obtained during full inspiration with the patient in tical software (Stata, version 14, StataCorp).
the prone position. Histopathologic Evaluation and Radiologic-
Chest CT scans were evaluated by consensus by Pathologic Correlation Results
two dedicated thoracic radiologists who had 32 and For 74 of the 136 CT scans, a pathologic sample Near-equal numbers of men and women
11 years of thoracic imaging experience and were was available for assessment within 1 year of the were included in the study (50.7% of the pa-
blinded to other data. CT scans were scored for scored CT scan. Pathologic samples from surgical tients were women). The mean patient age
the presence of reticulation, honeycombing, trac- lung biopsies were reviewed by a pulmonary pa- was 63.5 ± 10.9 years.
tion bronchiectasis, air trapping or mosaic atten- thologist with expertise in ILD, as reported else-
uation, and ground-glass opacity. The preponder- where [7]. The biopsy specimens were evaluated CT Findings
ant distribution of lung disease was also scored in for pathologic patterns of ILD, such as UIP, NSIP, The mean lung volume affected by ILD
zonal plane (i.e., diffuse, upper, middle, or lower) organizing pneumonia, lymphocytic interstitial was 22.5% ± 12.5%. Most subjects had basi-
and transverse plane (i.e., diffuse, bronchovascu- pneumonitis, and chronic HP, as well as for other lar (89.0%; 121/136) and peripheral (73.5%;
lar, peripheral, or peripheral with subpleural spar- evidence of underlying autoimmune diseases 100/136) predominant disease distribution.
ing). Reticulation, honeycombing, traction bron- Diffuse distribution was the next most com-
chiectasis, air trapping or mosaic attenuation, and Statistical Analysis mon pattern in both the zonal (8.7%) and axial
ground-glass opacity were scored as present or ab- CT findings were descriptively summarized (15.1%) planes. Approximately 60.2% of sub-
sent on CT; the percentage of lung involvement as mean (± SD) values or median (range) values, jects had honeycombing on CT. In those with
AJR:208, June 2017 1231
Chung et al.
TABLE 1: Usual Interstitial subjects, who had a mean affected lung vol- 2). Nearly one-tenth of the subjects had an
Pneumonitis (UIP) Patterns ume of 12.1% ± 5.6%. Almost all subjects imaging pattern that was most consistent
on CT Scans of 136 had traction bronchiectasis (96.3%; 131/136), with HP, rather than the typical CT patterns
Patients With Interstitial with a mean affected lung volume of 11.4% ± ascribed to CTD-associated ILD.
Pneumonia With Men and smokers or former smokers had a
7.1%. Multicompartment involvement, as de-
Autoimmune Features
fined by IPAF criteria, was common. Pleural UIP pattern more often than the pattern that
Downloaded from www.ajronline.org by 125.167.114.159 on 05/24/21 from IP address 125.167.114.159. Copyright ARRS. For personal use only; all rights reserved
CT UIP Pattern No. (%) of Patients effusion or thickening was present in 13.2% was inconsistent with UIP on chest CT (Table
UIP 70 (51.5)
of subjects (18/136), and pericardial effusion 3). Subjects with the UIP pattern on CT were
or thickening was present in 1.5% (2/136). also older than those with a pattern inconsis-
Possible UIP 19 (14.0)
Mosaic attenuation without CT evidence of tent with UIP on CT. No apparent difference
Inconsistent with UIP 47 (34.6) emphysema was present in 34.6% of subjects related to race was noted, although this may
(47/136), and pulmonary artery enlargement have been a function of limited power.
TABLE 2: CT Patterns for 136 was present in 27.2% (37/136).
Patients With I nterstitial CT and Pathologic Correlation
Pneumonia With Usual Interstitial Pneumonitis Pattern and The strongest agreement between CT and
Autoimmune Features Diagnosis on CT pathologic findings, with regard to UIP diag-
No. (%) of Most subjects with IPAF had a UIP or pos- nosis, occurred when CT scans were scored as
CT Pattern Patients sible UIP pattern (65.4%; 89/136) on CT (Ta- having a UIP pattern (93.8% of these subjects
ble 1). A substantially smaller number of sub- had UIP diagnosed on the basis of pathologic
Usual interstitial pneumonitis 70 (51.5)
jects had a pattern inconsistent with UIP on findings). There was slightly lower agreement
NSIP 37 (27.2) CT (34.6%; 47/136). The most common CT between CT and pathologic findings when CT
Hypersensitivity pneumonitis 11 (8.1) finding (53.2%; 25/47) on CT scans with a scans were scored as having a possible UIP
NSIP organizing pneumonia 9 (6.6) pattern inconsistent with UIP was the pres- pattern on CT (83.3% of these subjects had
ence of a significant degree of ground-glass UIP diagnosed on the basis of pathologic find-
Organizing pneumonia 5 (3.7)
opacity. Nonbasilar predominant distribution ings), although this was not statistically differ-
Other 4 (2.9) of disease, nonperipheral predominant distri- ent when compared with CT scans with a UIP
Note—NSIP = nonspecific interstitial pneumonia. bution, or both distributions were noted on pattern on CT (Table 3). There was much low-
23.4% (11/47) of CT scans that showed a pat- er agreement between CT findings and patho-
honeycombing, the mean lung volume affect- tern inconsistent with UIP. logic findings when CT scans were scored
ed was 3.1% ± 4.3%. Ground-glass opacity On the basis of the imaging pattern only, as having a pattern inconsistent with UIP (or
was present in 27.9% of subjects, for whom UIP was the single best diagnosis for approx- 50.0% UIP according to pathologic findings).
the mean lung volume affected was 15.9% ± imately one-half of the subjects, followed by When compared with the other CT categories,
17.1%. Air trapping was present in 10.3% of NSIP for one-quarter of the subjects (Table a statistically significant difference was noted
in the concordance of CT findings and patho-
TABLE 3: Demographic Characteristics of Patients With I nterstitial logic findings in subjects with a pattern incon-
Pneumonia With Autoimmune Features Relative to sistent with UIP (p < 0.001).
High-Confidence CT Diagnoses
Survival and CT Findings
Pattern Inconsistent With UIP on CT Univariate statistically significant CT
Characteristic (n = 47) UIP Pattern on CT (n = 70) p
findings that were associated with worse sur-
Smoker 19 (40.4) 42 (60.0) 0.041a vival included the percentage of reticulation
White race 31 (66.0) 51 (72.9) 0.537 (hazard ratio [HR], 1.04; 95% CI, 1.01–1.06),
Male 16 (34.0) 41 (58.6) 0.014a the presence of honeycombing (HR, 2.60;
95% CI, 1.33–5.07), mosaic attenuation cor-
Age (y), mean ± SD 59.4 ± 11.5 66.7 ± 9.5 < 0.001a
rected for the presence of emphysema (HR,
Note—Except where noted otherwise, data are number (%) of patients. UIP = usual interstitial pneumonitis.
aStatistically significant.
2.17; 95% CI, 1.19–3.95), and pulmonary ar-
tery enlargement (HR, 2.23; 95% CI, 1.22–
4.05) (Table 4). The UIP pattern on CT and
TABLE 4: Radiologic and Pathologic Correlation for Diagnosis of Usual the distribution of pulmonary fibrosis were
Interstitial Pneumonitis (UIP)
not statistically significant predictors of sur-
No. of Patients With Pathologic Diagnosis vival. Corresponding Kaplan-Meier survival
Patients With UIP curves with log-rank test p values are shown
CT Diagnosis Not UIP UIP Diagnosis (%)
for the presence on CT of honeycombing,
Inconsistent with UIP 12 12 50.0 mosaic attenuation corrected for the pres-
Possible UIP 3 15 83.3 ence of emphysema, and pulmonary artery
UIP 2 30 93.8
enlargement in Figures 4, 5, and 6, respec-
tively. Focused multivariate analysis showed
Total 17 57
that only honeycombing (HR, 2.17; 95% CI,
1232 AJR:208, June 2017
CT Findings, Radiologic-Pathologic Correlation, and Predictors of Survival for Patients With IPAF
100 100
75 75
Survival Rate (%)
Survival Rate (%)
50 50
Downloaded from www.ajronline.org by 125.167.114.159 on 05/24/21 from IP address 125.167.114.159. Copyright ARRS. For personal use only; all rights reserved
25 25
0 0
0 24 48 72 96 120 0 24 48 72 96 120
Time (mo) Time (mo)
Fig. 4—Survival of patients with interstitial pneumonia with autoimmune features Fig. 5—Survival of patients with interstitial pneumonia with autoimmune features
with honeycombing on CT versus those without honeycombing on CT. Kaplan- with mosaic attenuation on CT versus those without mosaic attenuation on CT.
Meier survival curves show that those with honeycombing on CT (dashed line) had Kaplan-Meier survival curves show that patients with mosaic attenuation on
significantly worse survival than those without honeycombing on CT (solid line) CT (dashed line) had significantly worse survival than those without mosaic
(p = 0.0092, log-rank test). attenuation on CT (solid line) (p = 0.0092, log-rank test).
100
75
Survival Rate (%)
50
25
Fig. 6—Survival of patients with interstitial pneumonia with autoimmune features
with pulmonary artery enlargement on CT versus those without pulmonary
0 artery enlargement on CT. Kaplan-Meier survival curves show that patients with
pulmonary artery enlargement of 3.3 cm or greater (dashed line) had significantly
0 12 24 36 48 60 72
Time (mo) worse survival than those with pulmonary artery enlargement of less than 3.3 cm
(solid line) (p = 0.0071, log-rank test).
1.05–4.47) and pulmonary artery enlarge- studies of UCTD have shown that UIP is the features [26]. In the present study, a similar
ment (HR, 2.08; 95% CI, 1.02–4.20) were in- most common pattern, although NSIP is also proportion of subjects with IPAF had a CT
dependent predictors of survival, but the per- quite common, depending on the diagnostic cri- pattern consistent with HP. Although not di-
centage of reticulation and the presence of teria used [2, 4, 22, 23]. In patients with CTD, agnostic of HP (which requires multidisci-
mosaic attenuation corrected for emphysema NSIP is the most common type of lung disease. plinary discussion), our findings suggest that
on CT were not (Table 5). An exception to this rule is rheumatoid ar- there is relationship between autoimmunity
thritis, for which the UIP pattern is most com- and HP, whether pathophysiologic or pheno-
Discussion mon [24, 25]. The high prevalence of the UIP typic. Only a small number of subjects ex-
The present study had five primary find- pattern in patients with IPAF suggests that posed to antigens known to cause HP have
ings. First, contrary to our initial hypothesis, these patients may mimic patients with rheu- significant ILD develop, implying the pres-
most subjects with IPAF had a UIP pattern matoid arthritis with regard to their underly- ence of an underlying genetic susceptibil-
of pulmonary fibrosis on CT. Second, one of ing pathophysiologic profile and prognosis. ity. Inhaled substances may trigger auto-
10 subjects with IPAF had an imaging pat- This subject is worthy of future investigation. immune disease in susceptible individuals,
tern that was most consistent with HP. Third, In our cohort, a history of smoking, older age, because development of CTD has been re-
older age, smoking, and male sex were asso- and male sex were more likely characteristics ported in individuals exposed to cigarette
ciated with a UIP pattern. Fourth, a possi- of patients with a UIP pattern of pulmonary smoke, silica, and coal dust, in addition to
ble UIP pattern on CT is strongly associated fibrosis, compared with patients with a pat- dust and chemicals from the attacks on the
with UIP on pathologic analysis. Fifth, hon- tern inconsistent with UIP. For patients with World Trade Center on September 11, 2001
eycombing and pulmonary artery enlarge- idiopathic pulmonary fibrosis, smoking, older [26–30]. Alternatively, although the CT ap-
ment on CT were independent predictors of patient age, and male sex are major risk fac- pearance of IPAF has yet to be formally de-
survival for patients with IPAF. tors for the development of UIP [5]. Similar fined, morphologic findings of HP may be
In the current study, a UIP or possible UIP phenomena may be present in patients with one of the phenotypes of IPAF. In addition,
pattern on CT was present in most subjects with IPAF and should be explored further. there may be yet-undefined IPAF imaging
IPAF (65.4%). Recent evidence suggests that The presence of autoimmune features patterns, as has been suggested by the sub-
most patients with a possible UIP pattern on CT in patients with HP has only recently been stantially small number of subjects whose
have UIP on pathologic analysis, as do those formally recognized; up to 15% of patients CT findings could not be classified into tra-
with a UIP pattern on CT [13, 19–21]. Previous with HP may have associated autoimmune ditional UIP categories.
AJR:208, June 2017 1233
Chung et al.
TABLE 5: Cox Unadjusted and Adjusted Analyses of Prognostic Features Noted on High-Resolution CT Examinations
of Patients With Interstitial Pneumonia With Autoimmune Features
Unadjusted Analysis (n = 136) Adjusted Analysisa (n = 136)
Variable HR p 95% CI HR p 95% CI
Downloaded from www.ajronline.org by 125.167.114.159 on 05/24/21 from IP address 125.167.114.159. Copyright ARRS. For personal use only; all rights reserved
Honeycomb pattern 2.60 0.005 1.33–5.07 2.17 0.037 1.05–4.47
Reticulation (% involvement) 1.04 0.001 1.01–1.06 1.01 0.386 0.98–1.05
Multicompartment features
Mosaic attenuation excluding emphysemab 2.17 0.011 1.19–3.95 1.79 0.117 0.87–3.70
Pulmonary artery enlargementc 2.23 0.009 1.22–4.05 2.08 0.043 1.02–4.20
UIP patternd
Possible UIP 0.99 0.982 0.36–2.73
Definite UIP 1.57 0.172 0.82–2.98
Mosaic attenuation 1.63 0.102 0.91–2.94
Ground-glass opacities 0.99 0.968 0.52–1.88
Axial distribution of fibrosise
Peripheral 1.40 0.575 0.43–4.56
Peripheral with subpleural sparing 0.32 0.325 0.03–3.09
Diffuse 1.29 0.722 0.32–5.17
Pleural or pericardial effusion or thickening 1.77 0.146 0.82–3.81
Note—HR = hazard ratio, UIP = usual interstitial pneumonitis. Statistically significant values are shown in boldface type.
a Adjusted for age, sex, forced vital capacity, diffusing capacity of the lung for carbon monoxide, and presence of clinical domain.
bFor multicompartment features, with patients with a history of smoking excluded, univariate analysis revealed an HR of 1.83 (p = 0.047).
cWith use of a pulmonary artery diameter cutoff of 33 mm.
dCompared with pattern inconsistent with UIP.
eCompared with central distribution, bronchovascular distribution, or both.
Multiple previous studies in different clin- finitive diagnosis. Given the morbidity and was somewhat unexpected. NSIP is associ-
ical settings have shown that a CT pattern mortality risks associated with surgical lung ated with survival superior to that associated
that is suggestive of UIP but does not meet biopsy performed for patients with ILD, an with UIP in the idiopathic setting [33, 34].
strict criteria for UIP is almost always asso- alternative pathway that minimizes the num- Therefore, one would expect patients with a
ciated with a UIP pattern on pathologic anal- ber of patients sent for surgical lung biopsy high-confidence UIP pattern on CT to have
ysis [14, 19, 20, 31]. In 96 patients with his- is attractive. Our data and previous studies worse survival than patients with a pattern
tologically proven UIP or NSIP, Flaherty et suggest that, rather than have patients with inconsistent with UIP on CT.
al. [14] showed that all 11 patients with prob- a possible UIP pattern on CT undergo biop- However, previous studies suggest that
able UIP on HRCT (defined as CT findings sy, such patients could be managed like those the clinical significance of the UIP pattern
consistent with UIP except for the absence with a high-confidence UIP pattern on CT. in the setting of CTD is less certain. In a
of basilar distribution) had UIP diagnosed The ramifications of the IPAF classifica- heterogeneous group of subjects with CTD,
on pathologic analysis. Another study, which tion with regard to survival have yet to be no significant difference in survival was
was part of a larger genomewide association fully delineated. Studies evaluating prog- noted between patients with CTD-related
study, showed that, in 82.4% of cases, proba- nostic factors in UCTD (or similar designa- NSIP and UIP [35]. Bouros et al. [36] noted
ble UIP (defined as CT findings suggestive of tions) have suggested that patients with auto- little difference in the survival of patients
UIP but with honeycombing absent) was as- immune interstitial pneumonias who do not with systemic sclerosis–related ILD with
sociated with a UIP diagnosis on pathologic meet strict criteria for a defined CTD likely NSIP, compared with those with UIP (91%
analysis [13]. In two separate studies of idio- have a survival rate similar to that of patients vs 82%, respectively).
pathic pulmonary fibrosis, Raghu et al. [20] with idiopathic pulmonary fibrosis and may Conversely, a small study of patients with
and Yagihashi et al. [19] found that 94.0% have worse survival than those with defined rheumatoid arthritis showed that patients
of 84 subjects and 93.8% of 64 subjects, re- CTD [2–4]. In the current study, the pres- with UIP have worse survival than those with
spectively, who met CT criteria for possible ence of honeycombing on CT was indepen- NSIP, on the basis of pathologic findings, al-
UIP had UIP confirmed on the basis of his- dently associated with worse survival, which though the much higher prevalence of smok-
tologic findings. These findings suggest that supports the well-accepted relationship be- ing among patients with UIP, compared with
these cases may not require biopsy for accu- tween disease severity and poor survival in patients with NSIP, may have been a con-
rate diagnosis. Current guidelines direct pa- patients with pulmonary fibrosis [6, 32]. On founding factor [37]. An imaging-based study
tients with a possible UIP pattern on CT to the other hand, the absence of a survival dif- of patients with rheumatoid arthritis showed
undergo surgical lung biopsy for more de- ference relative to CT classification of UIP that patients with a definite UIP pattern on
1234 AJR:208, June 2017
CT Findings, Radiologic-Pathologic Correlation, and Predictors of Survival for Patients With IPAF
CT had worse survival, compared with pa- agnosis and treatment of ILD; therefore, our 10. Lynch DA, Austin JH, Hogg JC, et al. CT-defin-
tients without this CT pattern (median surviv- results may not be generalizable to the com- able subtypes of chronic obstructive pulmonary
al, 3.2 vs 6.6 years, respectively) [25]. Sim- munity setting. disease: a statement of the Fleischner Society.
ilarly, Solomon et al. [24] showed that, for This study shows that a UIP pattern was Radiology 2015; 277:192–205
patients with rheumatoid arthritis, the pres- present on CT for most subjects with IPAF 11. Tan RT, Kuzo R, Goodman LR, Siegel R, Haasler
ence of the UIP pattern on CT was associated and that it was more common among those GB, Presberg KW. Utility of CT scan evaluation
Downloaded from www.ajronline.org by 125.167.114.159 on 05/24/21 from IP address 125.167.114.159. Copyright ARRS. For personal use only; all rights reserved
with worse survival than was presence of the with known risk factors for idiopathic pul- for predicting pulmonary hypertension in patients
NSIP pattern on CT, although this finding did monary fibrosis (e.g., older age, smoking his- with parenchymal lung disease. Medical College
not persist after multivariate analysis. tory, and male sex). A possible UIP pattern of Wisconsin Lung Transplant Group. Chest 1998;
Our results also suggest that pulmonary on CT was almost always associated with 113:1250–1256
artery size on CT is independently associ- UIP on pathologic analysis. Also, a HP pat- 12. Edwards PD, Bull RK, Coulden R. CT measure-
ated with worse survival for patients with tern on CT was not rare in our cohort with ment of main pulmonary artery diameter. Br J
IPAF. Pulmonary hypertension is a known IPAF, which implies the possible presence of Radiol 1998; 71:1018–1020
manifestation of CTDs and has poor prog- a relationship between autoimmunity and HP. 13. Chung JH, Chawla A, Peljto AL, et al. CT scan
nostic ramifications [38]. Extensive literature Further research regarding CT phenotypes in findings of probable usual interstitial pneumonitis
exists that documents the strong correlation the setting of IPAF will be necessary to deter- have a high predictive value for histologic usual
between pulmonary artery size on CT and mine the significance of this finding. Final- interstitial pneumonitis. Chest 2015; 147:450–459
pulmonary hypertension [12, 39]. The most ly, honeycombing and pulmonary artery en- 14. Flaherty KR, Thwaite EL, Kazerooni EA, et al.
likely theory for our result is that pulmonary largement on CT are independent predictors Radiological versus histological diagnosis in UIP
artery size is associated with pulmonary hy- of poor survival for patients with IPAF. and NSIP: survival implications. Thorax 2003;
pertension, which is, in turn, associated with 58:143–148
poor prognosis. This theory could not be for- References 15. Sumikawa H, Johkoh T, Fujimoto K, et al. Patho-
mally tested because of the observational na- 1. Kinder BW, Collard HR, Koth L, et al. Idiopathic logically proved nonspecific interstitial pneumo-
ture of the present study. However, little, if nonspecific interstitial pneumonia: lung manifesta- nia: CT pattern analysis as compared with usual
any, correlation exists between CT pulmo- tion of undifferentiated connective tissue disease? interstitial pneumonia CT pattern. Radiology
nary artery measurements and pulmonary Am J Respir Crit Care Med 2007; 176:691–697 2014; 272:549–556
hypertension in the setting of pulmonary fi- 2. Corte TJ, Copley SJ, Desai SR, et al. Significance of 16. Silva CI, Müller NL, Lynch DA, et al. Chronic hy-
brosis, particularly if pulmonary fibrosis is connective tissue disease features in idiopathic inter- persensitivity pneumonitis: differentiation from
more severe, possibly because of alterations stitial pneumonia. Eur Respir J 2012; 39:661–668 idiopathic pulmonary fibrosis and nonspecific in-
in mediastinal structures secondary to un- 3. Fischer A, Pfalzgraf FJ, Feghali-Bostwick CA, et terstitial pneumonia by using thin-section CT.
derlying chronic pulmonary pathologic find- al. Anti-th/to-positivity in a cohort of patients Radiology 2008; 246:288–297
ings [11, 40, 41]. Therefore, considering alter- with idiopathic pulmonary fibrosis. J Rheumatol 17. Chung JH, Peljto AL, Chawla A, et al. CT pheno-
native pathophysiologic mechanisms would 2006; 33:1600–1605 types of pulmonary fibrosis in the MUC5B pro-
be prudent. The ratio of pulmonary artery 4. Vij R, Noth I, Strek ME. Autoimmune-featured moter site polymorphism. Chest 2016; 149:1215–
size to aorta size on CT has been strongly as- interstitial lung disease: a distinct entity. Chest 1222
sociated with acute exacerbations in a large 2011; 140:1292–1299 18. Ley B, Ryerson CJ, Vittinghoff E, et al. A multidi-
cohort with chronic obstructive pulmonary 5. Raghu G, Collard HR, Egan JJ, et al. An official mensional index and staging system for idiopathic
disease with external validation [42]. In the ATS/ERS/JRS/ALAT statement: idiopathic pul- pulmonary fibrosis. Ann Intern Med 2012;
setting of chronic lung disease, enlargement monary fibrosis—evidence-based guidelines for 156:684–691
of the pulmonary artery on CT may signal diagnosis and management. Am J Respir Crit 19. Yagihashi K, Huckleberry J, Colby TV, et al. Ra-
an increased likelihood for pulmonary exac- Care Med 2011; 183:788–824 diologic-pathologic discordance in biopsy-proven
erbations and, eventually, pulmonary-related 6. Lynch DA, Godwin JD, Safrin S, et al. High-reso- usual interstitial pneumonia. Eur Respir J 2016;
death, although this is speculative. lution computed tomography in idiopathic pulmo- 47:1189–1197
The limitations of the present study in- nary fibrosis: diagnosis and prognosis. Am J 20. Raghu G, Lynch D, Godwin JD, et al. Diagnosis of
clude its retrospective design and its rela- Respir Crit Care Med 2005; 172:488–493 idiopathic pulmonary fibrosis with high-resolu-
tively small number of subjects, which may 7. Oldham JM, Adegunsoye A, Valenzi E, et al. tion CT in patients with little or no radiological
have limited the power of the study. Howev- Characterisation of patients with interstitial pneu- evidence of honeycombing: secondary analysis of
er, the total number of subjects is on par with monia with autoimmune features. Eur Respir J a randomised, controlled trial. Lancet Respir Med
the number of subjects in other single-center 2016; 47: 1767–1775 2014; 2:277–284
studies of CTD-related ILD. Also, there was 8. Fischer A, Antoniou KM, Brown KK, et al. An 21. Gruden JF, Panse PM, Gotway MB, Jensen EA,
some heterogeneity in CT acquisition param- official European Respiratory Society/American Wellnitz CV, Wesselius L. Diagnosis of usual in-
eters, given that some of the CT scans were Thoracic Society research statement: interstitial terstitial pneumonitis in the absence of honey-
not performed at our medical center. We ad- pneumonia with autoimmune features. Eur Respir combing: evaluation of specific CT criteria with
dressed this issue by only scoring CT scans J 2015; 46: 976–987 clinical follow-up in 38 patients. AJR 2016;
from outside hospitals, which could be accu- 9. Kuriyama K, Gamsu G, Stern RG, Cann CE, 206:472–480
rately analyzed for findings of pulmonary fi- Herfkens RJ, Brundage BH. CT-determined pul- 22. Omote N, Taniguchi H, Kondoh Y, et al. Lung-
brosis. Finally, this study was performed at a monary artery diameters in predicting pulmonary dominant connective tissue disease: clinical, ra-
tertiary medical center specializing in the di- hypertension. Invest Radiol 1984; 19:16–22 diologic, and histologic features. Chest 2015;
AJR:208, June 2017 1235
Chung et al.
148:1438–1446 case-control study of selected systemic autoim- pathologic subsets of fibrosing alveolitis in pa-
23. Kim HC, Ji W, Kim MY, et al. Interstitial pneumo- mune diseases in World Trade Center rescue/re- tients with systemic sclerosis and their relation-
nia related to undifferentiated connective tissue covery workers. Arthritis Rheumatol 2015; ship to outcome. Am J Respir Crit Care Med
disease: pathologic pattern and prognosis. Chest 67:1369–1376 2002; 165:1581–1586
2015; 147:165–172 31. Hunninghake GW, Lynch DA, Galvin JR, et al. 37. Lee HK, Kim DS, Yoo B, et al. Histopathologic
24. Solomon JJ, Chung JH, Cosgrove GP, et al. Pre- Radiologic findings are strongly associated with a pattern and clinical features of rheumatoid arthri-
Downloaded from www.ajronline.org by 125.167.114.159 on 05/24/21 from IP address 125.167.114.159. Copyright ARRS. For personal use only; all rights reserved
dictors of mortality in rheumatoid arthritis-asso- pathologic diagnosis of usual interstitial pneumo- tis-associated interstitial lung disease. Chest
ciated interstitial lung disease. Eur Respir J 2016; nia. Chest 2003; 124:1215–1223 2005; 127:2019–2027
47:588–596 32. Sumikawa H, Johkoh T, Colby TV, et al. Comput- 38. Condliffe R, Kiely DG, Peacock AJ, et al. Con-
25. Kim EJ, Elicker BM, Maldonado F, et al. Usual ed tomography findings in pathological usual in- nective tissue disease-associated pulmonary arte-
interstitial pneumonia in rheumatoid arthritis-as- terstitial pneumonia: relationship to survival. rial hypertension in the modern treatment era.
sociated interstitial lung disease. Eur Respir J Am J Respir Crit Care Med 2008; 177:433–439 Am J Respir Crit Care Med 2009; 179:151–157
2010; 35:1322–1328 33. Nicholson AG, Colby TV, du Bois RM, Hansell 39. Alhamad EH, Al-Boukai AA, Al-Kassimi FA, et al.
26. Adegunsoye A, OldhAm JM, Demchuk C, Montner DM, Wells AU. The prognostic significance of the Prediction of pulmonary hypertension in patients
S, Vij R, Strek ME. Predictors of survival in coexis- histologic pattern of interstitial pneumonia in pa- with or without interstitial lung disease: reliability
tent hypersensitivity pneumonitis with autoimmune tients presenting with the clinical entity of crypto- of CT findings. Radiology 2011; 260:875–883
features. Respir Med 2016; 114:53–60 genic fibrosing alveolitis. Am J Respir Crit Care 40. Devaraj A, Wells AU, Meister MG, Corte TJ, Wort
27. Doyle TJ, Dellaripa PF, Batra K, et al. Functional Med 2000; 162:2213–2217 SJ, Hansell DM. Detection of pulmonary hyperten-
impact of a spectrum of interstitial lung abnormali- 34. Daniil ZD, Gilchrist FC, Nicholson AG, et al. A sion with multidetector CT and echocardiography
ties in rheumatoid arthritis. Chest 2014; 146:41–50 histologic pattern of nonspecific interstitial pneu- alone and in combination. Radiology 2010;
28. Kart L, Sarikaya S, Gurel A, et al. Rheumatoid monia is associated with a better prognosis than 254:609–616
factor seropositivity and rheumatoid symptoms in usual interstitial pneumonia in patients with cryp- 41. Zisman DA, Karlamangla AS, Ross DJ, et al.
coal worker’s pneumoconiosis. Clin Rheumatol togenic fibrosing alveolitis. Am J Respir Crit Care High-resolution chest CT findings do not predict
2003; 22:365–366 Med 1999; 160:899–905 the presence of pulmonary hypertension in ad-
29. Rocha MC, Santos LM, Bagatin E, et al. Genetic 35. Park JH, Kim DS, Park IN, et al. Prognosis of fi- vanced idiopathic pulmonary fibrosis. Chest
polymorphisms and surface expression of CTLA-4 brotic interstitial pneumonia: idiopathic versus 2007; 132:773–779
and PD-1 on T cells of silica-exposed workers. Int collagen vascular disease-related subtypes. Am J 42. Wells JM, Washko GR, Han MK, et al. Pulmonary
J Hyg Environ Health 2012; 215:562–569 Respir Crit Care Med 2007; 175:705–711 arterial enlargement and acute exacerbations of
30. Webber MP, Moir W, Zeig-Owens R, et al. Nested 36. Bouros D, Wells AU, Nicholson AG, et al. Histo- COPD. N Engl J Med 2012; 367:913–921
1236 AJR:208, June 2017
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Modern Technology of Radiation PhysicsDocument67 pagesThe Modern Technology of Radiation PhysicsNaomi Morales Medina0% (1)
- MRI BasicsDocument192 pagesMRI BasicsCruise Films ProductionsNo ratings yet
- Glossary of Implant Dentistry 3 ICOIDocument106 pagesGlossary of Implant Dentistry 3 ICOINAGARAJNo ratings yet
- Introduction To The Topographical Anatomy and Operative SurgeryDocument43 pagesIntroduction To The Topographical Anatomy and Operative SurgeryKavan Vyas100% (1)
- CTDocument3 pagesCTsameh dra100% (1)
- User Manual Accuchek ERS MeterDocument39 pagesUser Manual Accuchek ERS MeterBashir Ahmad100% (5)
- 3D Virtual Treatment Planning of Orthognathic Surgery A Step-By-Step Approach For Orthodontists and SurgeonsDocument580 pages3D Virtual Treatment Planning of Orthognathic Surgery A Step-By-Step Approach For Orthodontists and SurgeonsAbad Salcedo100% (5)
- Radiology Notes (1-36)Document83 pagesRadiology Notes (1-36)el spin artifactNo ratings yet
- Basics of FractureDocument12 pagesBasics of Fracturecimahmudraju100% (2)
- Case Study - FractureDocument35 pagesCase Study - FractureJo-anne Cordero100% (3)
- 2019 Article 1273Document17 pages2019 Article 1273Ahmad Fari Arief LopaNo ratings yet
- Long-Term Control of Macular Edema With Adalimumab After Cataract Surgery in A Japanese Child With Juvenile Idiopathic Arthritis: Case Report and Review of 26 Japanese PatientsDocument10 pagesLong-Term Control of Macular Edema With Adalimumab After Cataract Surgery in A Japanese Child With Juvenile Idiopathic Arthritis: Case Report and Review of 26 Japanese PatientsAhmad Fari Arief LopaNo ratings yet
- Rare Fungal Infection Linked To A Case of Juvenile ArthritisDocument9 pagesRare Fungal Infection Linked To A Case of Juvenile ArthritisAhmad Fari Arief LopaNo ratings yet
- Image Quality of Prospectively ECG-Triggered Coronary CT Angiography in Heart Transplant RecipientsDocument6 pagesImage Quality of Prospectively ECG-Triggered Coronary CT Angiography in Heart Transplant RecipientsAhmad Fari Arief LopaNo ratings yet
- CT Findings of Pneumonia After Lung TransplantationDocument8 pagesCT Findings of Pneumonia After Lung TransplantationAhmad Fari Arief LopaNo ratings yet
- Jurnal 20Document5 pagesJurnal 20Ahmad Fari Arief LopaNo ratings yet
- Jurnal 4Document8 pagesJurnal 4Ahmad Fari Arief LopaNo ratings yet
- COVID-19 Pneumonia: A Pictorial Review of CT Findings and Differential DiagnosisDocument8 pagesCOVID-19 Pneumonia: A Pictorial Review of CT Findings and Differential DiagnosisAhmad Fari Arief LopaNo ratings yet
- Jurnal 1Document6 pagesJurnal 1Ahmad Fari Arief LopaNo ratings yet
- Referat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Document14 pagesReferat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Ahmad Fari Arief LopaNo ratings yet
- Journal Reading BartholinithisDocument21 pagesJournal Reading BartholinithisAhmad Fari Arief LopaNo ratings yet
- Gastro Graf in Oral Rectal SuspDocument13 pagesGastro Graf in Oral Rectal SuspnirmalscribdNo ratings yet
- DR. JAIME T. CRUZ, Petitioner, vs. FELICISIMO V. AGAS, JR., RespondentDocument2 pagesDR. JAIME T. CRUZ, Petitioner, vs. FELICISIMO V. AGAS, JR., RespondentKaren Joy MasapolNo ratings yet
- Puting and Applications Advanced Techniques For Clinical DentistryDocument407 pagesPuting and Applications Advanced Techniques For Clinical DentistryKyaw Swe Shin MyintNo ratings yet
- Quality Use of AI in Medical Imaging-What Do Radiologists Need To Know?Document8 pagesQuality Use of AI in Medical Imaging-What Do Radiologists Need To Know?SANDEEP REDDYNo ratings yet
- A Case Study of DIBH To Spare Abdominal Organs at Risk For Renal Cell Carcinoma MR-Guided RadiotherapyDocument14 pagesA Case Study of DIBH To Spare Abdominal Organs at Risk For Renal Cell Carcinoma MR-Guided Radiotherapyapi-525837437No ratings yet
- Journal of Biomedical Informatics: Dynamic Deformable Attention Network (Ddanet) For Semantic SegmentationDocument319 pagesJournal of Biomedical Informatics: Dynamic Deformable Attention Network (Ddanet) For Semantic SegmentationKumar RajamaniNo ratings yet
- Distraction Osteogenesis As Followed by CT Scan in Pierre Robin SequenceDocument8 pagesDistraction Osteogenesis As Followed by CT Scan in Pierre Robin SequenceMauricio Alejandro Maureira CifuentesNo ratings yet
- International Journal of Radiology and Imaging Technology Ijrit 8 089Document4 pagesInternational Journal of Radiology and Imaging Technology Ijrit 8 089khalizamaulinaNo ratings yet
- Book Reading: Dr. Francisco Gilbert Timothy Dr. Adam Moeljono, SP - OT (K) SpineDocument21 pagesBook Reading: Dr. Francisco Gilbert Timothy Dr. Adam Moeljono, SP - OT (K) SpineFrancisco GaniNo ratings yet
- Acute Appendicitis in PregnancyDocument18 pagesAcute Appendicitis in Pregnancynicholas Rojas SIlvaNo ratings yet
- Case 25-2020: A 47-Year-Old Woman With A Lung Mass: Case Records Massachusetts General HospitalDocument10 pagesCase 25-2020: A 47-Year-Old Woman With A Lung Mass: Case Records Massachusetts General HospitalClinica CorominasNo ratings yet
- Quick Company Analysis Dr. Lal Pathlabs Limited: ShikshaDocument13 pagesQuick Company Analysis Dr. Lal Pathlabs Limited: ShikshaRishu GautamNo ratings yet
- Sample PET Report 1Document2 pagesSample PET Report 1Samir S. ShahNo ratings yet
- Case Studies On Additive ManufacturingDocument8 pagesCase Studies On Additive Manufacturingrohan_murdeshwar100% (1)
- PET CT Principles PDFDocument28 pagesPET CT Principles PDFIonuț RusNo ratings yet
- Sector409056 PDFDocument467 pagesSector409056 PDFVictor BogdanNo ratings yet
- Malignant Parotid Tumor ImagingDocument11 pagesMalignant Parotid Tumor ImagingTuan NguyenNo ratings yet
- Role of Multi-Detector CT Venography in Evaluation of Pelvic Congestion SyndromeDocument7 pagesRole of Multi-Detector CT Venography in Evaluation of Pelvic Congestion SyndromeAhmed Sayed AwadNo ratings yet
- Acceptance Testing CTDocument8 pagesAcceptance Testing CTpanzerdyayNo ratings yet
- Head Orientation in CBCT-generated CephalogramsDocument7 pagesHead Orientation in CBCT-generated CephalogramsBinta Bhirawa AnoragaNo ratings yet