
You might also like
- Rapid Review of Embryology, First PDFDocument137 pagesRapid Review of Embryology, First PDFmayurdadhaniya100% (1)
- The Upper Extremity: Sufitni Megasari SitorusDocument37 pagesThe Upper Extremity: Sufitni Megasari SitorusFakhrur RaziNo ratings yet
- General Embryology PDFDocument9 pagesGeneral Embryology PDFmedpgnotesNo ratings yet
- Gynecology Notes Ebook PDFDocument51 pagesGynecology Notes Ebook PDFThistell Thistle100% (1)
- Clinical Anatomy by Systems Richard S Sne - 59cca2b31723ddac3bb48043Document4 pagesClinical Anatomy by Systems Richard S Sne - 59cca2b31723ddac3bb48043Triana0% (1)
- A&P - 6. Pelvic & Lower Limb Detailed Anatomy (42p)Document42 pagesA&P - 6. Pelvic & Lower Limb Detailed Anatomy (42p)andreeaNo ratings yet
- 2-Pelvic Walls, Joints, Vessels & NervesDocument32 pages2-Pelvic Walls, Joints, Vessels & NervesAbdul Rafay ShaikhNo ratings yet
- Ankle and FootDocument206 pagesAnkle and FootZenabNaaz100% (1)
- Self Assessment & Review ObstetricsDocument535 pagesSelf Assessment & Review ObstetricsUmniyah Abu-NaylaNo ratings yet
- Jigjiga University: Anatomy of PerineumDocument114 pagesJigjiga University: Anatomy of PerineumKamal AhmedNo ratings yet
- Anatomy Upper Limb Sameh DossDocument143 pagesAnatomy Upper Limb Sameh DossStella JNo ratings yet
- EmbryologyDocument68 pagesEmbryologyانس ابوهيبةNo ratings yet
- Blood Physiology 2022Document116 pagesBlood Physiology 2022Gurmessa FekaduNo ratings yet
- Gynaecology Revision PDFDocument13 pagesGynaecology Revision PDFAadhi AadhiNo ratings yet
- Pediatric Urology HDocument54 pagesPediatric Urology HAlaa A. AbdelrahimNo ratings yet
- Biomechanics NotesDocument21 pagesBiomechanics Notesstarlight9394100% (1)
- Etiology of Pelvic Organ ProlapseDocument9 pagesEtiology of Pelvic Organ ProlapseAlandey e TatianaNo ratings yet
- PPP LarynxDocument65 pagesPPP LarynxAnkur MittalNo ratings yet
- Kadasne's Textbook of Embryology PDFDocument380 pagesKadasne's Textbook of Embryology PDFBharath Magesh100% (1)
- Pelvic Floor Anatomy and The Surgery of Pulsion EnterocoeleDocument185 pagesPelvic Floor Anatomy and The Surgery of Pulsion EnterocoeleSamir CastilloNo ratings yet
- EmbryologyDocument26 pagesEmbryologyBryan Mae H. Degorio100% (2)
- A. A. Allen The Price of Gods Miracle Working PowerDocument52 pagesA. A. Allen The Price of Gods Miracle Working Powerprijiv86% (7)
- Urinary Incontinence HandoutDocument6 pagesUrinary Incontinence HandoutGautam ReddyNo ratings yet
- PHYSIOLOGYDocument10 pagesPHYSIOLOGYapi-1986354875% (4)
- Abdomen - IntroductionDocument63 pagesAbdomen - IntroductionPriyanka SharmaNo ratings yet
- Blood Supply Pelvic OrgansDocument39 pagesBlood Supply Pelvic OrgansoliviaNo ratings yet
- Ginecologia Women's Imaging Obstetrics and GynecologyDocument199 pagesGinecologia Women's Imaging Obstetrics and GynecologyAnca LoyolaNo ratings yet
- AMORC What Constitutes A High Degree Member in AMORC 2Document3 pagesAMORC What Constitutes A High Degree Member in AMORC 2Francis EjikeNo ratings yet
- Livro Vertex MACIOCIADocument62 pagesLivro Vertex MACIOCIAxandinhag100% (5)
- Anatomy Notes Week3Document18 pagesAnatomy Notes Week3Zainab Ali100% (1)
- Dr. Reynaldo V. Lopez Senior Lecturer Department of AnatomyDocument55 pagesDr. Reynaldo V. Lopez Senior Lecturer Department of AnatomyMohammad AliNo ratings yet
- ALSO ManualDocument466 pagesALSO Manualemkay1234No ratings yet
- Pelvic AnatomyDocument0 pagesPelvic AnatomyAlynne De Luna PascuaNo ratings yet
- Jaypee Gold Standard Mini Atlas Series® Embryology (2010) (PDF) (UnitedVRG)Document217 pagesJaypee Gold Standard Mini Atlas Series® Embryology (2010) (PDF) (UnitedVRG)reyod0% (1)
- PADI Rescue Diver - Blank Knowledge ReviewDocument13 pagesPADI Rescue Diver - Blank Knowledge ReviewAj Quek67% (3)
- AnatomyDocument74 pagesAnatomyhafeez khanNo ratings yet
- 01-System Devices Configuration - Rev GDocument36 pages01-System Devices Configuration - Rev GPABITRA PATRANo ratings yet
- Lecture 7 - Physiology of LaborDocument30 pagesLecture 7 - Physiology of LaborMelissa Aina Mohd Yusof100% (1)
- Notes Breast Anatomy and PhysiologyDocument35 pagesNotes Breast Anatomy and PhysiologySoufiane ElKostali100% (2)
- Applied Anatomy of Upper Limb Part OneDocument66 pagesApplied Anatomy of Upper Limb Part Oneprinceej100% (3)
- 637a1d3f56493 - Anatomy Fun Easy Summary - of - AbdomenDocument64 pages637a1d3f56493 - Anatomy Fun Easy Summary - of - AbdomenPA inbox100% (2)
- Neck LumpDocument18 pagesNeck LumpJosh BurkeNo ratings yet
- Moore's Clinically Oriented Anatomy 6th EdDocument4 pagesMoore's Clinically Oriented Anatomy 6th EdJohna Pauline Mandac67% (6)
- Atlas de Anatomia Anthony B. OlingerDocument52 pagesAtlas de Anatomia Anthony B. OlingerKatia Roxana Quispe CondoriNo ratings yet
- Colposcopy in Gyn PracticeDocument59 pagesColposcopy in Gyn PracticeJoseph Kimaro100% (1)
- SEPLOS 48V 100A BMS User Manual: Shenzhen Seplos Technology Co.,LtdDocument30 pagesSEPLOS 48V 100A BMS User Manual: Shenzhen Seplos Technology Co.,LtdDennis Go100% (2)
- Colorectal Oral Boards ReviewDocument79 pagesColorectal Oral Boards Revieweztouch12No ratings yet
- Ifth DitionDocument25 pagesIfth DitionAlfie Omega0% (1)
- ESSENTIALS OF HUMAN EMBRYOLOGY by Prof NGASSAPADocument315 pagesESSENTIALS OF HUMAN EMBRYOLOGY by Prof NGASSAPAJumbe Mohamed100% (3)
- Tourism Law CompleteDocument225 pagesTourism Law CompleteDennis Go100% (4)
- Items of Work For RoadsDocument6 pagesItems of Work For Roadsjhc1123No ratings yet
- Hinmans+Atlas+of+UroSurgical+Anatomy Nodrm PDFDocument381 pagesHinmans+Atlas+of+UroSurgical+Anatomy Nodrm PDFMariya Lyashevych100% (1)
- Embryology and Anatomy of The Gastrointestinal TractDocument58 pagesEmbryology and Anatomy of The Gastrointestinal TractYitancloudNo ratings yet
- PROLOG: Obstetrics, Ninth Edition (Assessment & Critique)From EverandPROLOG: Obstetrics, Ninth Edition (Assessment & Critique)No ratings yet
- Atlas of Pelvic SurgeryDocument3 pagesAtlas of Pelvic SurgeryYoanne Homecillo0% (1)
- A Primer: Series of 2014Document25 pagesA Primer: Series of 2014Dennis GoNo ratings yet
- First Aid Q&A EmbryologyDocument13 pagesFirst Aid Q&A EmbryologyzyadNo ratings yet
- Histology Exam IV Review Part 2Document26 pagesHistology Exam IV Review Part 2ashdmb217No ratings yet
- TestesDocument39 pagesTestesImadShaheen50% (2)
- Some Basic Concepts in EmbryologyDocument13 pagesSome Basic Concepts in EmbryologyDr Md Abedur Rahman100% (3)
- 1-Indroduction To EmbryologyDocument25 pages1-Indroduction To Embryologyselman P k100% (1)
- Anatomy SBA MCQ eMRCSDocument81 pagesAnatomy SBA MCQ eMRCSTowhid HasanNo ratings yet
- Reproductive PhysiologyDocument40 pagesReproductive PhysiologyBaiq Trisna Satriana100% (1)
- Slipped Capital Femoral EpiphysisDocument21 pagesSlipped Capital Femoral EpiphysisJulián RincónNo ratings yet
- Bones of Upper and Lower Limbs - RevisionDocument15 pagesBones of Upper and Lower Limbs - RevisionChess Nuts100% (1)
- Anatomi PelvisDocument44 pagesAnatomi Pelvisari naNo ratings yet
- Abdomen 2Document41 pagesAbdomen 2Cristina-Alexandra ConstantinNo ratings yet
- Ultrasound - A GuideDocument9 pagesUltrasound - A GuideDebasish KunduNo ratings yet
- Parent 20 Deephouse 20200720 JBE20 Stakeholder 20 Id 20 and 20 SalienceDocument24 pagesParent 20 Deephouse 20200720 JBE20 Stakeholder 20 Id 20 and 20 SalienceDennis GoNo ratings yet
- DBA 009 - Legal AspectsDocument8 pagesDBA 009 - Legal AspectsDennis GoNo ratings yet
- SA Deye Manual 2 1Document41 pagesSA Deye Manual 2 1Dennis GoNo ratings yet
- Wuxi Zozo New Energy Technology Co., LTD: Add:Bldg. 3, No. 99, Qingshuroad Binhu District, Wuxi, Jiangsu, ChinaDocument4 pagesWuxi Zozo New Energy Technology Co., LTD: Add:Bldg. 3, No. 99, Qingshuroad Binhu District, Wuxi, Jiangsu, ChinaDennis GoNo ratings yet
- PV Grid Tie Inverter: User ManualDocument21 pagesPV Grid Tie Inverter: User ManualDennis GoNo ratings yet
- Syllabus Tourism Laws CKSCDocument6 pagesSyllabus Tourism Laws CKSCDennis Go50% (2)
- Murder ArgumentDocument2 pagesMurder ArgumentDennis GoNo ratings yet
- Assignment 33 PDFDocument9 pagesAssignment 33 PDFsayan mukherjeeNo ratings yet
- Numerology 666 Meaning: What Angel Number 666 REALLY Means!Document2 pagesNumerology 666 Meaning: What Angel Number 666 REALLY Means!LlNo ratings yet
- 4K Resolution: The Future of ResolutionsDocument15 pages4K Resolution: The Future of ResolutionsRavi JoshiNo ratings yet
- 15b. FANC - Focused Antenatal Care - Koros E.KDocument71 pages15b. FANC - Focused Antenatal Care - Koros E.KMercy KeruboNo ratings yet
- Modules With Available Quota - 2019!11!12 - 9amDocument7 pagesModules With Available Quota - 2019!11!12 - 9amdhmanoharNo ratings yet
- Catchment CharacterisationDocument48 pagesCatchment CharacterisationSherlock BaileyNo ratings yet
- Berkeley To San JoseDocument88 pagesBerkeley To San JoseTimothy HightowerNo ratings yet
- Chapter 34 - The Influence of Monetary and Fiscal Policy On Aggregate Demand (Compatibility Mode) PDFDocument19 pagesChapter 34 - The Influence of Monetary and Fiscal Policy On Aggregate Demand (Compatibility Mode) PDFthanhvu78No ratings yet
- NUMBERS 2 Percentage ChangeDocument2 pagesNUMBERS 2 Percentage ChangeDinangaNo ratings yet
- Health Group3Document29 pagesHealth Group3Angela OrenseNo ratings yet
- Appendix 2-4.ep31422 - g-16Document15 pagesAppendix 2-4.ep31422 - g-16bsnegi111No ratings yet
- Reglas Digitales Mitutoyo Scale Units Linear ScalesDocument31 pagesReglas Digitales Mitutoyo Scale Units Linear ScalesAngelmambrinNo ratings yet
- Proline Table-Top Machines Z005 Up To Z100: Product InformationDocument2 pagesProline Table-Top Machines Z005 Up To Z100: Product InformationErika Mae EnticoNo ratings yet
- s1160 Jorvet Infusion PumpDocument4 pagess1160 Jorvet Infusion PumpGhulam HyderNo ratings yet
- WBMDocument90 pagesWBMMiguel RegisNo ratings yet
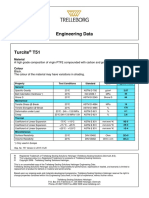
- Turcite T51 Engineering DataDocument1 pageTurcite T51 Engineering DataAntonio Rivera VillavicencioNo ratings yet
- Design and Modeling of Zvs Resonantsepic Converter For High FrequencyapplicationsDocument8 pagesDesign and Modeling of Zvs Resonantsepic Converter For High FrequencyapplicationsMohamed WarkzizNo ratings yet
- A Proposal Study On The Construction of An Automated People Mover APM Inside The New Manila International Airport NMIADocument78 pagesA Proposal Study On The Construction of An Automated People Mover APM Inside The New Manila International Airport NMIAMckyle FaustinoNo ratings yet
- [Download pdf] Mastering Microsoft Fabric Saasification Of Analytics 1St Edition Debananda Ghosh online ebook all chapter pdfDocument42 pages[Download pdf] Mastering Microsoft Fabric Saasification Of Analytics 1St Edition Debananda Ghosh online ebook all chapter pdflinda.coles284100% (11)
- Saga of Hundred Years of Hardinge Bridge: A. GhoshalDocument15 pagesSaga of Hundred Years of Hardinge Bridge: A. GhoshalAnonymous L90AMktANo ratings yet
- AUSMAT Student Guide 2011Document16 pagesAUSMAT Student Guide 2011Sunway UniversityNo ratings yet
- Syllabus: Survey Training Institute, H-8/2 IslamabadDocument7 pagesSyllabus: Survey Training Institute, H-8/2 Islamabadsajid khanNo ratings yet
- GFRC Floating Concrete Hearth For Concrete Wood FiDocument11 pagesGFRC Floating Concrete Hearth For Concrete Wood FiJuliano. PQMNo ratings yet


























































































![[Download pdf] Mastering Microsoft Fabric Saasification Of Analytics 1St Edition Debananda Ghosh online ebook all chapter pdf](https://imgv2-2-f.scribdassets.com/img/document/732592422/149x198/f876884e8e/1716289284?v=1)



