You might also like
- Cardiology NotesDocument13 pagesCardiology NotesFreeNursingNotes78% (9)
- Neem by Ellen NortenDocument100 pagesNeem by Ellen NortenMano DrabuzeliaiNo ratings yet
- MOH Pocket Manual in Emergency Medicine PDFDocument244 pagesMOH Pocket Manual in Emergency Medicine PDFErandi Andrea100% (2)
- U WORLD (Step 1) – INFECTIOUS DISEASES + MICROBIOLOGY (EDUCATIONAL OBJECTIVESDocument75 pagesU WORLD (Step 1) – INFECTIOUS DISEASES + MICROBIOLOGY (EDUCATIONAL OBJECTIVESDrbee10No ratings yet
- BlsDocument62 pagesBlspaediatrica89% (19)
- Approach To Chest PainDocument48 pagesApproach To Chest PainIslam ElsayedNo ratings yet
- Dilated Cardiomyopathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDilated Cardiomyopathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Nursing Mnemonics: The Ultimate Tips and Notes For NursesFrom EverandNursing Mnemonics: The Ultimate Tips and Notes For NursesRating: 5 out of 5 stars5/5 (1)
- Lifting Vs Volumizing-The Difference in Facial Minimally Invasive Procedures When Respecting The Line of LigamentsDocument7 pagesLifting Vs Volumizing-The Difference in Facial Minimally Invasive Procedures When Respecting The Line of LigamentsArcelino Farias100% (1)
- Care of Patient With Respiratory DisordersDocument35 pagesCare of Patient With Respiratory Disorderskriiteeabns100% (1)
- 9 MedicineDocument351 pages9 MedicineSaravan PramodNo ratings yet
- Myocardial InfarctionDocument4 pagesMyocardial InfarctionLetecia MooreNo ratings yet
- Internal Medicine 1, Conrad FischerDocument35 pagesInternal Medicine 1, Conrad Fischerdukelist566100% (3)
- (Cancer Drug Discovery and Development) Ulrike S. Stein PhD, Wolfgang Walther PhD, Peter M. Schlag MD, PhD (Auth.), Peter M. Schlag MD, Ulrike Stein PhD, Alexander M. M. Eggermont MD, PhD (Eds.)-RegioDocument455 pages(Cancer Drug Discovery and Development) Ulrike S. Stein PhD, Wolfgang Walther PhD, Peter M. Schlag MD, PhD (Auth.), Peter M. Schlag MD, Ulrike Stein PhD, Alexander M. M. Eggermont MD, PhD (Eds.)-RegioEsteban Gonzàlez RodriguezNo ratings yet
- Cardiac Biomarker PresentationDocument29 pagesCardiac Biomarker PresentationMohana PreeshaNo ratings yet
- Myocardial Infarction. BPTDocument62 pagesMyocardial Infarction. BPTAanchal GuptaNo ratings yet
- Ecg 01Document103 pagesEcg 01Bandar al ghamdi100% (1)
- Breaking The Silence - Art TherapyDocument43 pagesBreaking The Silence - Art TherapyAdriana100% (1)
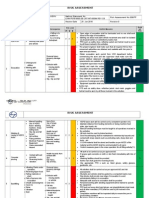
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- Cardiac BiomarkersDocument72 pagesCardiac BiomarkersAmey JatharNo ratings yet
- Anaesthesia For Renal TransplantationDocument65 pagesAnaesthesia For Renal TransplantationSouvik MaitraNo ratings yet
- 3 MDRRMC SampleDocument57 pages3 MDRRMC SampleMakoy Salonga100% (2)
- MOH Pocket Manual in Emergency MedicineDocument244 pagesMOH Pocket Manual in Emergency MedicineAli Al-Brahim (AlucardAli)No ratings yet
- CDRH Learn Module-GCP 101 - Lacorte PDFDocument21 pagesCDRH Learn Module-GCP 101 - Lacorte PDFVelasco JohnNo ratings yet
- Risk For Infection Related To Presence of Surgical Wounds As Evidenced by MER 2nd DegreeDocument3 pagesRisk For Infection Related To Presence of Surgical Wounds As Evidenced by MER 2nd DegreeSenyorita KHaye75% (12)
- Cardiac Care and ManagementDocument38 pagesCardiac Care and ManagementJoyce SiosonNo ratings yet
- Myocardial InfarctionDocument40 pagesMyocardial InfarctionHIRANGER100% (3)
- Signs, Symptoms and Treatment of Acute Myocardial InfarctionDocument53 pagesSigns, Symptoms and Treatment of Acute Myocardial InfarctionAngnaKalsiNo ratings yet
- Dedication 1Document8 pagesDedication 1Mego PlamoniaNo ratings yet
- Care and Management of The Client With Cardiac Alterations: Presented By: Jessaly Joyce SiosonDocument38 pagesCare and Management of The Client With Cardiac Alterations: Presented By: Jessaly Joyce SiosonJoyce SiosonNo ratings yet
- Professional Growth and DevelopmentDocument154 pagesProfessional Growth and DevelopmentNina Anne Paracad100% (3)
- Grizz Phys Tier 2 PDFDocument19 pagesGrizz Phys Tier 2 PDFJ VivianNo ratings yet
- DMLC Part I & II Cyprus (Hyundai Busan)Document17 pagesDMLC Part I & II Cyprus (Hyundai Busan)Shankar Singh0% (1)
- Acute Coronary SyndromeDocument30 pagesAcute Coronary SyndromeEndar EszterNo ratings yet
- Updates On Acute Coronary SyndromeDocument121 pagesUpdates On Acute Coronary SyndromeDwi Akbarina YahyaNo ratings yet
- Biochemical Makers of Cardiac DiseaseDocument45 pagesBiochemical Makers of Cardiac DiseaseSalman RashidNo ratings yet
- CardiacDocument37 pagesCardiacmeghanaNo ratings yet
- Bio MarkersDocument19 pagesBio MarkersassumptaNo ratings yet
- Pathogenesis of Cardiac DisordersDocument28 pagesPathogenesis of Cardiac DisordersUdochukwu EnebeNo ratings yet
- Coronary Artery DiseaseDocument32 pagesCoronary Artery DiseasecjissamNo ratings yet
- Myocardial Infarction: Maj Aswathy Ganesh I Year MSC (N) Con, AfmcDocument45 pagesMyocardial Infarction: Maj Aswathy Ganesh I Year MSC (N) Con, AfmcAswathy ganeshNo ratings yet
- Coronary Artery Disease: By. Saiha AlinaDocument19 pagesCoronary Artery Disease: By. Saiha AlinasaihaNo ratings yet
- Acute Management of StrokeDocument19 pagesAcute Management of StrokeBKGUBIONo ratings yet
- Acute Coronary Syndrome: Dr. Isbandiyah, SPPDDocument22 pagesAcute Coronary Syndrome: Dr. Isbandiyah, SPPDMohammad SutamiNo ratings yet
- Acute Miocard InfarkDocument32 pagesAcute Miocard InfarkhansNo ratings yet
- Myocardial Infarction (MI) Definition and ManagementDocument33 pagesMyocardial Infarction (MI) Definition and ManagementArchana GaonkarNo ratings yet
- Nursing Mangement Client With Myocardial Infarction (Mi) Heart AttackDocument35 pagesNursing Mangement Client With Myocardial Infarction (Mi) Heart AttackTania Febria AzizahNo ratings yet
- Acute Coronary SyndromeDocument41 pagesAcute Coronary SyndromeAbdulhameed MohamedNo ratings yet
- Diagnosis of AMI: Biochemical Markers of Myocardial InjuryDocument11 pagesDiagnosis of AMI: Biochemical Markers of Myocardial InjuryHisham AlhirereNo ratings yet
- Acs 235Document39 pagesAcs 235api-3815243No ratings yet
- ACS LectureDocument55 pagesACS LectureAyunda AlmiradaniNo ratings yet
- ACS Types & TreatmentDocument613 pagesACS Types & Treatmentyangi dokaNo ratings yet
- Aspartate Aminotransferase (AST, Serum GlutamicDocument11 pagesAspartate Aminotransferase (AST, Serum GlutamicLeo RinaldiNo ratings yet
- 9 CsaDocument34 pages9 Csaمحمد بن الصادقNo ratings yet
- Stress Testing in Cardiac EvaluationDocument15 pagesStress Testing in Cardiac EvaluationKanak SoniNo ratings yet
- Pharmacotherapy for ACS ManagementDocument71 pagesPharmacotherapy for ACS ManagementABREHAM BUKULONo ratings yet
- Acute Coronary SyndrommeDocument50 pagesAcute Coronary SyndrommeAndriani Kemala SariNo ratings yet
- Heart Tests Explained: Cardiac Biomarkers, ECG, Stress Testing & MoreDocument25 pagesHeart Tests Explained: Cardiac Biomarkers, ECG, Stress Testing & MoreClaire GidoNo ratings yet
- Blackshear - Chest Pain ContrastDocument13 pagesBlackshear - Chest Pain ContrastMazen SalamaNo ratings yet
- Acute Myocardial InfarctionDocument22 pagesAcute Myocardial InfarctionkpsuanNo ratings yet
- Myocardial InfarctionDocument34 pagesMyocardial InfarctionMeera ANN AJINo ratings yet
- 11-Acs2 StemiDocument33 pages11-Acs2 Stemiمحمد بن الصادقNo ratings yet
- Myocardial Infarction Diagnosis and TreatmentDocument22 pagesMyocardial Infarction Diagnosis and TreatmentSrijana MahatoNo ratings yet
- Cardiac Rehabilitation Case Study ExplainedDocument20 pagesCardiac Rehabilitation Case Study Explainedعادل خليلNo ratings yet
- P ('t':'3', 'I':'669636497') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document56 pagesP ('t':'3', 'I':'669636497') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Muna NadiNo ratings yet
- TROPONIN T & I Cardiac EnzymesDocument2 pagesTROPONIN T & I Cardiac EnzymesIanNo ratings yet
- Cardiovascular Lecture Notes: AnginaDocument23 pagesCardiovascular Lecture Notes: AnginaAnonymous iG0DCOfNo ratings yet
- Cardiovascular Case: Presented By: Dr. SyahrianiDocument30 pagesCardiovascular Case: Presented By: Dr. SyahrianiAkbar IskandarNo ratings yet
- Drug-Induced Arrhythmia TreatmentDocument27 pagesDrug-Induced Arrhythmia TreatmentLoiseNo ratings yet
- Pre Hospital and Initial Management of Acute CoronaryDocument33 pagesPre Hospital and Initial Management of Acute CoronaryYudo PradanaNo ratings yet
- Enzim CardiovascularDocument64 pagesEnzim Cardiovascularandre kesumaNo ratings yet
- Stroke, Inc IcpDocument6 pagesStroke, Inc IcpJojo JustoNo ratings yet
- Fast Facts for Patients: Thrombotic Thrombocytopenic Purpura: Prompt action saves livesFrom EverandFast Facts for Patients: Thrombotic Thrombocytopenic Purpura: Prompt action saves livesNo ratings yet
- Stability of Suspension Formulations of LansoprazoDocument7 pagesStability of Suspension Formulations of LansoprazoUmair MazharNo ratings yet
- Ehsaas Uni ListDocument6 pagesEhsaas Uni ListMuhammad arsalanNo ratings yet
- 9 - New Drug Development PlanDocument27 pages9 - New Drug Development PlanUmair MazharNo ratings yet
- Orig 1 S 000 Med RDocument84 pagesOrig 1 S 000 Med RUmair MazharNo ratings yet
- Article DistributionChannels EJSRDocument8 pagesArticle DistributionChannels EJSRUmair MazharNo ratings yet
- Invitro Dissolution Studies of Lansoprazole EC Pellets 12% W/W - A Comparative Dissolution Profile With Reference SampleDocument7 pagesInvitro Dissolution Studies of Lansoprazole EC Pellets 12% W/W - A Comparative Dissolution Profile With Reference SampleUmair MazharNo ratings yet
- Formulation and in Vitro Evaluation of LansoprazolDocument12 pagesFormulation and in Vitro Evaluation of LansoprazolUmair MazharNo ratings yet
- Vacancy Announcement: Sr. # Post Numbers of Posts Eligibility CriteriaDocument1 pageVacancy Announcement: Sr. # Post Numbers of Posts Eligibility CriteriaShariq WaheedNo ratings yet
- Formulation and Evaluation of Lansoprazole Delayed Release PelletsDocument20 pagesFormulation and Evaluation of Lansoprazole Delayed Release PelletsUmair MazharNo ratings yet
- Portal ManualDocument52 pagesPortal ManualsohaibNo ratings yet
- Orig 1 S 000 Med RDocument84 pagesOrig 1 S 000 Med RUmair MazharNo ratings yet
- Presented by : Vaishali G. Mohadikar Vinita G. PatelDocument31 pagesPresented by : Vaishali G. Mohadikar Vinita G. PatelUmair MazharNo ratings yet
- HEC ASA Eligibility ServiceDocument4 pagesHEC ASA Eligibility ServiceUmair MazharNo ratings yet
- GelDocument16 pagesGelUmair MazharNo ratings yet
- HEC ASA Eligibility ServiceDocument4 pagesHEC ASA Eligibility ServiceUmair MazharNo ratings yet
- Final Project R2Document112 pagesFinal Project R2Umair MazharNo ratings yet
- Questionnaire About Survey of Pharmaceutical Care in Community PharmaciesDocument4 pagesQuestionnaire About Survey of Pharmaceutical Care in Community PharmaciesUmair MazharNo ratings yet
- Portal ManualDocument52 pagesPortal ManualsohaibNo ratings yet
- Final Project R2Document112 pagesFinal Project R2Umair MazharNo ratings yet
- Final Project R2Document112 pagesFinal Project R2Umair MazharNo ratings yet
- Final Project R2Document112 pagesFinal Project R2Umair MazharNo ratings yet
- Portal ManualDocument52 pagesPortal ManualsohaibNo ratings yet
- Drug Targets and Design TechniquesDocument32 pagesDrug Targets and Design TechniquesUmair MazharNo ratings yet
- HEC ASA Eligibility ServiceDocument4 pagesHEC ASA Eligibility ServiceUmair MazharNo ratings yet
- Presented by : Vaishali G. Mohadikar Vinita G. PatelDocument31 pagesPresented by : Vaishali G. Mohadikar Vinita G. PatelUmair MazharNo ratings yet
- Presented by : Vaishali G. Mohadikar Vinita G. PatelDocument31 pagesPresented by : Vaishali G. Mohadikar Vinita G. PatelUmair MazharNo ratings yet
- Lung Cancer Signs, Types, DiagnosisDocument44 pagesLung Cancer Signs, Types, DiagnosisUmair MazharNo ratings yet
- Tuberculosis PPT Group #8Document43 pagesTuberculosis PPT Group #8Umair MazharNo ratings yet
- Effectiveness of A Functional Rehabilitation Program For Upper Limb Apraxia in Poststroke Patients: A Randomized Controlled TrialDocument11 pagesEffectiveness of A Functional Rehabilitation Program For Upper Limb Apraxia in Poststroke Patients: A Randomized Controlled Trialguohong huNo ratings yet
- Unit 1Document15 pagesUnit 1kunalNo ratings yet
- Hospital Self Assement ToolkitDocument28 pagesHospital Self Assement ToolkitNidhi VijanNo ratings yet
- Nursing Care Plan for Patient SafetyDocument9 pagesNursing Care Plan for Patient SafetyACOB, Jamil C.No ratings yet
- Plant Tissue Culture Media PDFDocument3 pagesPlant Tissue Culture Media PDFTitan Biotech100% (1)
- Radam, Sandralane C., Journal ReviewDocument3 pagesRadam, Sandralane C., Journal ReviewSandralane C. RadamNo ratings yet
- Trays PDFDocument18 pagesTrays PDFBilal Hasan100% (1)
- T2anklearthrodesis Optech b1000044d0710Document36 pagesT2anklearthrodesis Optech b1000044d0710Alsed GjoniNo ratings yet
- Top 5 Consumer Court CasesDocument7 pagesTop 5 Consumer Court CasesTanishka SoniNo ratings yet
- 1992 2007 Kpds Ilgisiz Cumle Sorulari Seyfihocacom - Pdf.pdfsifreDocument24 pages1992 2007 Kpds Ilgisiz Cumle Sorulari Seyfihocacom - Pdf.pdfsifreozgurekinsuNo ratings yet
- Petroleum Gases, Liquefied Petroleum Gas: IdentificationDocument4 pagesPetroleum Gases, Liquefied Petroleum Gas: IdentificationdigecaNo ratings yet
- Connectors 2Document14 pagesConnectors 2Irene SánchezNo ratings yet
- EBM TerbaruDocument5 pagesEBM TerbaruTetty PrasetyaNo ratings yet
- MSDSDocument3 pagesMSDSSiti Nurjanah SeptianiNo ratings yet
- Introduction To The Alpaca andDocument9 pagesIntroduction To The Alpaca andMai Chi PhạmNo ratings yet
- Veteran Resource Guide For Congressional District 9Document27 pagesVeteran Resource Guide For Congressional District 9RepSinemaNo ratings yet