You might also like
- Clinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareFrom EverandClinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareNo ratings yet
- RCCMDocument6 pagesRCCMJenny FitriaNo ratings yet
- 9019-Article Text-34483-1-10-20210724Document5 pages9019-Article Text-34483-1-10-20210724Brenda RodriguesNo ratings yet
- Ab in CopdDocument14 pagesAb in CopdDinar Danan SukmawatiNo ratings yet
- 127 411 1 SMDocument16 pages127 411 1 SMDario ToschiNo ratings yet
- Concise Clinical Review: Non-Cystic Fibrosis BronchiectasisDocument11 pagesConcise Clinical Review: Non-Cystic Fibrosis BronchiectasisJuwitaNo ratings yet
- Andrew Et AlDocument18 pagesAndrew Et AlmuarifNo ratings yet
- Management of Acute Exacerbation of Copd: Dr. Fanny WS KoDocument3 pagesManagement of Acute Exacerbation of Copd: Dr. Fanny WS KoCalca NeusNo ratings yet
- Copd Nihilismo BuenisimoDocument8 pagesCopd Nihilismo BuenisimoJose Lopez FuentesNo ratings yet
- Respiratory Tract Virus Infections in The Elderly With PneumoniaDocument11 pagesRespiratory Tract Virus Infections in The Elderly With PneumoniatanyasisNo ratings yet
- Comorbid AsthmaDocument12 pagesComorbid AsthmasaviraNo ratings yet
- Low 2018Document9 pagesLow 2018Hendri WahyudiNo ratings yet
- Arti Revi 11Document8 pagesArti Revi 11LuLu NikhlaturNo ratings yet
- Bronchiectasis - NonCFDocument10 pagesBronchiectasis - NonCFNiniek Iin FNo ratings yet
- Tuberculosis and Lung Damage: From Epidemiology To PathophysiologyDocument20 pagesTuberculosis and Lung Damage: From Epidemiology To PathophysiologyDyan TonyNo ratings yet
- Neumonia Asosiada A VentiladorDocument11 pagesNeumonia Asosiada A VentiladorYnomata RusamellNo ratings yet
- Respiratory Medicine: XDocument8 pagesRespiratory Medicine: XYuriz HkNo ratings yet
- Antoniu SA, Trofor AC - Inhaled Gentamicin in Non-Cystic Fibrosis Bronchiectasis Effects of Long-Term TherapyDocument4 pagesAntoniu SA, Trofor AC - Inhaled Gentamicin in Non-Cystic Fibrosis Bronchiectasis Effects of Long-Term TherapydanandonieNo ratings yet
- Acute Exacerbation of Chronic Obstructive Pulmonary DiseaseDocument5 pagesAcute Exacerbation of Chronic Obstructive Pulmonary Diseaseteguh sNo ratings yet
- AnnalsATS 201804-245OCDocument8 pagesAnnalsATS 201804-245OCMila KarmilaNo ratings yet
- Jurnal Perawatan PaliatifDocument16 pagesJurnal Perawatan Paliatifnurwanda hamidaNo ratings yet
- Full ArticleDocument8 pagesFull Articlekbrown733No ratings yet
- Estudio POST HOC Increase TreprostinilDocument10 pagesEstudio POST HOC Increase TreprostinilMaria Jose Contreras SilvaNo ratings yet
- Review ArdsDocument25 pagesReview ArdsAdel HamadaNo ratings yet
- Procalcitoninandcap PDFDocument10 pagesProcalcitoninandcap PDFmohd zonNo ratings yet
- Mortality BeDocument8 pagesMortality BeJaya Semara PutraNo ratings yet
- NIH Public Access: Author ManuscriptDocument14 pagesNIH Public Access: Author ManuscriptamorsantoNo ratings yet
- Pneumonia 3Document8 pagesPneumonia 3furqan92No ratings yet
- Comparative Risks of Chronic Inhaled Corticosteroids and Macrolides For BronchiectasisDocument11 pagesComparative Risks of Chronic Inhaled Corticosteroids and Macrolides For BronchiectasiskarlosNo ratings yet
- Adherence To Therapies in Cystic Fibrosis: A Targeted Literature ReviewDocument18 pagesAdherence To Therapies in Cystic Fibrosis: A Targeted Literature Reviewangelica barrazaNo ratings yet
- How Does Pseudomonas Aeruginosa Affect The Progression of Bronchiectasis - 1Document6 pagesHow Does Pseudomonas Aeruginosa Affect The Progression of Bronchiectasis - 1Brenda EstradaNo ratings yet
- Cystic Fibrosis - Management of Pulmonary Exacerbations - UpToDateDocument31 pagesCystic Fibrosis - Management of Pulmonary Exacerbations - UpToDateDylanNo ratings yet
- 431 2021 Article 4025Document9 pages431 2021 Article 4025Johan Wijaya KesitNo ratings yet
- Bronquiectasias Revision 2016 MEdicineDocument7 pagesBronquiectasias Revision 2016 MEdicinerecursitaNo ratings yet
- Ventilatory Strategies in Obstructive Lung. Parrilla2014Document10 pagesVentilatory Strategies in Obstructive Lung. Parrilla2014EzeBorjesNo ratings yet
- Cap AsmaDocument10 pagesCap AsmaAuliaNo ratings yet
- The Aetiology and Antibiotic Management of Community-Acquired Pneumonia in Adults in Europe: A Literature ReviewDocument15 pagesThe Aetiology and Antibiotic Management of Community-Acquired Pneumonia in Adults in Europe: A Literature ReviewPutu Sukma RadhanaNo ratings yet
- Chow 2015Document12 pagesChow 2015Isaias RamirezNo ratings yet
- Life 13 00459Document14 pagesLife 13 00459wulanesterNo ratings yet
- Pertanyaan 7Document14 pagesPertanyaan 7WicakNo ratings yet
- Joseph J. Zorc Caroline Breese Hall: Bronchiolitis: Recent Evidence On Diagnosis and Management, MD, Msce, ,, MDDocument10 pagesJoseph J. Zorc Caroline Breese Hall: Bronchiolitis: Recent Evidence On Diagnosis and Management, MD, Msce, ,, MDArie PrasetyowatiNo ratings yet
- NIEDERMAIER 2015 - Bronchopulmonary Dysplasia - An Overview About Pathophysiology ConceptsDocument7 pagesNIEDERMAIER 2015 - Bronchopulmonary Dysplasia - An Overview About Pathophysiology ConceptsRafael JustinoNo ratings yet
- Bronchiectasis ExacerbationDocument14 pagesBronchiectasis ExacerbationAriandindi AriandiNo ratings yet
- Pi Is 0012369216463579Document2 pagesPi Is 0012369216463579Nishant ShresthaNo ratings yet
- Title Sputum Bacteriology in Patients With Severe Chronic Lung DiseasesDocument47 pagesTitle Sputum Bacteriology in Patients With Severe Chronic Lung DiseasesHam FGNo ratings yet
- Evaluation of Antibiotics On Chronic Obstructive Pulmonary Disease Patient in Lung Hospital, West Sumatera, IndonesiaDocument4 pagesEvaluation of Antibiotics On Chronic Obstructive Pulmonary Disease Patient in Lung Hospital, West Sumatera, IndonesiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Disfagia Post Extubación Es Persistente y Asociada A Malos Resultados en Sobrevivientes de Enfermedades CriticasDocument9 pagesDisfagia Post Extubación Es Persistente y Asociada A Malos Resultados en Sobrevivientes de Enfermedades CriticasKatherine Lepe AbarcaNo ratings yet
- Perioperative Lung ProtectionDocument6 pagesPerioperative Lung ProtectionWilliamRayCassidyNo ratings yet
- Metoprolol y El EPOCDocument10 pagesMetoprolol y El EPOCMadyurit RamírezNo ratings yet
- Long-Term Azithromycin With Severe CopdDocument8 pagesLong-Term Azithromycin With Severe Copdlaksono_adeNo ratings yet
- MainDocument12 pagesMainMarly Tatiana Oviedo CaliNo ratings yet
- Pittsburgh Lung Conference: PneumoniaDocument4 pagesPittsburgh Lung Conference: PneumoniaYudha Rental'sNo ratings yet
- Acute Asthma Exacerbations: Phenotypes and Management: Charles B. Cairns, MD TDocument10 pagesAcute Asthma Exacerbations: Phenotypes and Management: Charles B. Cairns, MD TKaren Aguilar PalominoNo ratings yet
- Atm 09 05 390Document14 pagesAtm 09 05 390Adistha Eka Noveyani,No ratings yet
- 2019 - Chronic Obstructive Pulmonary Disease andDocument6 pages2019 - Chronic Obstructive Pulmonary Disease andAndreea MoalesNo ratings yet
- 1 s2.0 S1836955322001199 MainDocument8 pages1 s2.0 S1836955322001199 MainMarcin BystrowskiNo ratings yet
- Phenotypes Copd 2018Document10 pagesPhenotypes Copd 2018Angelica ChavesNo ratings yet
- Review Article: Acute Exacerbation of Chronic Obstructive Pulmonary Disease: Cardiovascular LinksDocument19 pagesReview Article: Acute Exacerbation of Chronic Obstructive Pulmonary Disease: Cardiovascular LinksMuhammad Jahari SupiantoNo ratings yet
- RecentprogressinthetreatmentofLN PDFDocument12 pagesRecentprogressinthetreatmentofLN PDFHosne araNo ratings yet
- Chronic TB Complications OutlineDocument15 pagesChronic TB Complications OutlineEver Seneca EscaLeraNo ratings yet
- bloodBLD2021012328 Suppl1Document5 pagesbloodBLD2021012328 Suppl1JOHN LOPERANo ratings yet
- Annals Int Med 1981 MOOP ABVDDocument5 pagesAnnals Int Med 1981 MOOP ABVDJOHN LOPERANo ratings yet
- Adult Outpatient Chemotherapy Order Form: Abvd Q28DaysDocument1 pageAdult Outpatient Chemotherapy Order Form: Abvd Q28DaysJOHN LOPERANo ratings yet
- Hodgkin Salv DALDocument9 pagesHodgkin Salv DALJOHN LOPERANo ratings yet
- Hodgkin OEPA-COPDACDocument7 pagesHodgkin OEPA-COPDACJOHN LOPERANo ratings yet
- Larotrectinib FIBROSARCOMA INFANTILDocument5 pagesLarotrectinib FIBROSARCOMA INFANTILJOHN LOPERANo ratings yet
- Advanced-Stagehodgkinlymphoma: by Joseph M. Connors, MDDocument5 pagesAdvanced-Stagehodgkinlymphoma: by Joseph M. Connors, MDJOHN LOPERANo ratings yet
- ABVD Vs QT Radiotherapy NEJM 2011Document10 pagesABVD Vs QT Radiotherapy NEJM 2011JOHN LOPERANo ratings yet
- Hepatoblastoma COG 0731 2009Document111 pagesHepatoblastoma COG 0731 2009milenaNo ratings yet
- Recomendacion de Lugano Pet CTDocument10 pagesRecomendacion de Lugano Pet CTJOHN LOPERANo ratings yet
- Evaluación RECIST 2008Document17 pagesEvaluación RECIST 2008JOHN LOPERANo ratings yet
- Biphenotypic Sinonasal Sarcoma: A Review and UpdateDocument6 pagesBiphenotypic Sinonasal Sarcoma: A Review and UpdateJOHN LOPERANo ratings yet
- Glioma Difuso de La Linea MediaDocument9 pagesGlioma Difuso de La Linea MediaJOHN LOPERANo ratings yet
- Linfoma Hodgkin Pet Scat Revision Lugano 2019Document6 pagesLinfoma Hodgkin Pet Scat Revision Lugano 2019JOHN LOPERANo ratings yet
- Gliomas Linea Media 1Document9 pagesGliomas Linea Media 1JOHN LOPERANo ratings yet
- Retinoblastoma Recaida RelapseDocument6 pagesRetinoblastoma Recaida RelapseJOHN LOPERANo ratings yet
- 2007 - Stem Cells of Ependymoma. NOCTH1Document5 pages2007 - Stem Cells of Ependymoma. NOCTH1JOHN LOPERANo ratings yet
- 2017 Article 279Document5 pages2017 Article 279JOHN LOPERANo ratings yet
- Jco Gliomas Bajo Grado 2017 BeatrizDocument9 pagesJco Gliomas Bajo Grado 2017 BeatrizJOHN LOPERANo ratings yet
- 2019 - Conformal Radiation Therapy For Pediatric Ependymoma, Chemotherapy For Incompletely Resected Ependymoma.Document13 pages2019 - Conformal Radiation Therapy For Pediatric Ependymoma, Chemotherapy For Incompletely Resected Ependymoma.JOHN LOPERANo ratings yet
- Wilms Tumor: Objectives Medical HistoryDocument7 pagesWilms Tumor: Objectives Medical HistoryJOHN LOPERANo ratings yet
- Protocolo GAMEC Germinal Relapse RecaidaDocument7 pagesProtocolo GAMEC Germinal Relapse RecaidaJOHN LOPERANo ratings yet
- Infections and Inflammations of The MouthDocument9 pagesInfections and Inflammations of The MouthSangeeta BSRNo ratings yet
- Cuong Vong - Resume - RevisedDocument2 pagesCuong Vong - Resume - Revisedapi-300295160No ratings yet
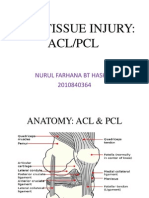
- Acl PCL PresentationDocument17 pagesAcl PCL PresentationSafwan Idham RamlanNo ratings yet
- Maja Musculo Sceletal-NovaDocument18 pagesMaja Musculo Sceletal-NovaLuka KoloskiNo ratings yet
- IntroductionDocument13 pagesIntroductionSaadNo ratings yet
- FIRST AID Is The Immediate Care Given To A Person Who Have Been Injured or Suddenly Taken IllDocument4 pagesFIRST AID Is The Immediate Care Given To A Person Who Have Been Injured or Suddenly Taken IllNat CatalanNo ratings yet
- Introduction To PathologyDocument40 pagesIntroduction To PathologyJugun HayatNo ratings yet
- Platelet Count Slide MethodDocument17 pagesPlatelet Count Slide MethodPrecious Yvanne PanagaNo ratings yet
- SarkopeniaDocument8 pagesSarkopeniaRamadhanaNo ratings yet
- History Taking and Examination For SurgeryDocument68 pagesHistory Taking and Examination For Surgerytayiba.m1995No ratings yet
- Case Study (Aub)Document16 pagesCase Study (Aub)Lucila Lugo0% (2)
- HAMP NCAL CompetencyModuleDocument47 pagesHAMP NCAL CompetencyModuleerlyNo ratings yet
- Introduction Maternity Pediatric Nursing 7th Leifer Test BankDocument12 pagesIntroduction Maternity Pediatric Nursing 7th Leifer Test Banksonyaaaq0% (1)
- Neuromuscular Blocking AgentsnewDocument22 pagesNeuromuscular Blocking Agentsnewvinay0717100% (1)
- Demncia Frontotemporal ContinumDocument25 pagesDemncia Frontotemporal ContinumcositaamorNo ratings yet
- Worksheet coronavirus-COVID-19-facts-and-adviceDocument4 pagesWorksheet coronavirus-COVID-19-facts-and-adviceF RengifoNo ratings yet
- Epidemiological Characterization of Dermatomycosis in EthiopiaDocument7 pagesEpidemiological Characterization of Dermatomycosis in EthiopiaMini LaksmiNo ratings yet
- Opioid Free Anesthesia A Different Regard To.98965 PDFDocument6 pagesOpioid Free Anesthesia A Different Regard To.98965 PDFgabriel herreraNo ratings yet
- A 22 Yrs Old Female With Progressive MuscleDocument25 pagesA 22 Yrs Old Female With Progressive MuscleTamzid Rabby TanmoyNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Implementation Rationale EvaluationDocument4 pagesNursing Care Plan: Assessment Diagnosis Planning Implementation Rationale Evaluationthomasfinley44No ratings yet
- Doctors at Greno-WestDocument4 pagesDoctors at Greno-WestAvik Kundu100% (1)
- Lap Pelayanan SeptemberDocument12 pagesLap Pelayanan SeptemberJosepb SimarmataNo ratings yet
- EpisiotomyDocument18 pagesEpisiotomyAnnapurna DangetiNo ratings yet
- Febrile Antigens Package InsertDocument2 pagesFebrile Antigens Package InsertAhmed AliNo ratings yet
- At HemoglobinDocument2 pagesAt HemoglobinzulfiNo ratings yet
- Lecturio 3755Document17 pagesLecturio 3755Pranjali WeladiNo ratings yet
- CH 067 Neonatal HypothermiaDocument10 pagesCH 067 Neonatal Hypothermiahelentika AvianaNo ratings yet
- Eco ModelDocument3 pagesEco ModelMary Joyce Juat DayotNo ratings yet
- Pregnancy and Birth Source BookDocument666 pagesPregnancy and Birth Source BookRaluca Horhat100% (3)
- Rakesh SainiDocument4 pagesRakesh SainiAdarsh SonkarNo ratings yet