You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Infection Control - NclexDocument4 pagesInfection Control - NclexTashaNo ratings yet
- Vitamin D SupplementsDocument11 pagesVitamin D SupplementsPetra JobovaNo ratings yet
- 7297 19768 4 PBDocument5 pages7297 19768 4 PBpujiindah lestariNo ratings yet
- Code Team Training and Assessment Best Practices From The Floor UCM - 486059Document34 pagesCode Team Training and Assessment Best Practices From The Floor UCM - 486059JoaoNo ratings yet
- Assessment of Quality of Movement During A Lateral Step-Down Test Narrative ReviewDocument9 pagesAssessment of Quality of Movement During A Lateral Step-Down Test Narrative ReviewCamila GuevaraNo ratings yet
- RESPIRE: A Spectral Kurtosis-Based Method To Extract Respiration Rate From Wearable PPG SignalsDocument6 pagesRESPIRE: A Spectral Kurtosis-Based Method To Extract Respiration Rate From Wearable PPG SignalsMariana Córdoba HolguínNo ratings yet
- Benign Essential Blepharospasm Information Page - National Institute of Neurological Disorders and StrokeDocument2 pagesBenign Essential Blepharospasm Information Page - National Institute of Neurological Disorders and StrokeJP OmerNo ratings yet
- International Consultation On Incontinence Questionnaire Short-Form (ICIQ-SF) para Incontinencia UrinariaDocument6 pagesInternational Consultation On Incontinence Questionnaire Short-Form (ICIQ-SF) para Incontinencia Urinariapeka_85No ratings yet
- An Experimental Study About The Amalgamation of Guajava of Guava Leaves Extract Shea Butter and Sandalwood As A Mosquito RepellentDocument96 pagesAn Experimental Study About The Amalgamation of Guajava of Guava Leaves Extract Shea Butter and Sandalwood As A Mosquito RepellentRob NoconNo ratings yet
- WNHS - OG.Arterial LineDocument17 pagesWNHS - OG.Arterial LinePurwadi SujalmoNo ratings yet
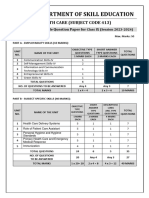
- 413 Health Care SQPDocument7 pages413 Health Care SQPAnil SarohaNo ratings yet
- Karen Clarke - BSDH PresentationDocument28 pagesKaren Clarke - BSDH PresentationWaheed UllahNo ratings yet
- Hypoglycemia Guidelines - AAP Vs PES (2172)Document12 pagesHypoglycemia Guidelines - AAP Vs PES (2172)Lina DiazNo ratings yet
- Y30stFZqSLY4yArZa3Ig - The Bison Brain Issue 1 Spring 2023Document10 pagesY30stFZqSLY4yArZa3Ig - The Bison Brain Issue 1 Spring 2023MED HAUSNo ratings yet
- NCM101j Quiz 2Document11 pagesNCM101j Quiz 2writingstuffforyou9No ratings yet
- Ms Word Notes - Template (May 2022)Document4 pagesMs Word Notes - Template (May 2022)Jaycee Anne AregloNo ratings yet
- Atheter Omenclature: R Freed A Urdaneta R Darflinger G VatakencherryDocument1 pageAtheter Omenclature: R Freed A Urdaneta R Darflinger G Vatakencherryamchoong100% (3)
- Introduction To Tungs Acupuncture PDFDocument323 pagesIntroduction To Tungs Acupuncture PDFBala Kiran Gaddam98% (48)
- Biology QuestionsDocument28 pagesBiology QuestionsShashi Kumar k KumarNo ratings yet
- Meat Processing Technology 1Document42 pagesMeat Processing Technology 1Abubakar Bello AliyuNo ratings yet
- ABG Tic Tac Toe CalculationDocument6 pagesABG Tic Tac Toe CalculationnatkwqNo ratings yet
- Effect of The Rho-Associated Kinase Inhibitor Eye Drop (Ripasudil) On Corneal Endothelial Wound HealingDocument9 pagesEffect of The Rho-Associated Kinase Inhibitor Eye Drop (Ripasudil) On Corneal Endothelial Wound HealingRaúl Plasencia SaliniNo ratings yet
- Instructions For Using The Wands of Horus - 2013Document48 pagesInstructions For Using The Wands of Horus - 2013har58100% (2)
- 19 Clinical - Assessment - of - Nutritional - StatusDocument9 pages19 Clinical - Assessment - of - Nutritional - StatusSamuel Kyei-BoatengNo ratings yet
- LupusQol Pour Evaluation de La Qualite de Vie Devilliers 2012 PDFDocument10 pagesLupusQol Pour Evaluation de La Qualite de Vie Devilliers 2012 PDFBamba DiawNo ratings yet
- DR - Azad A Haleem AL - Brefkani: University of Duhok Faculty of Medical Science School of Medicine Pediatrics DepartmentDocument58 pagesDR - Azad A Haleem AL - Brefkani: University of Duhok Faculty of Medical Science School of Medicine Pediatrics DepartmentGomathi ShankarNo ratings yet
- Catalogue Biosynex 2022 Export June Final PrintDocument52 pagesCatalogue Biosynex 2022 Export June Final PrintThiago GalloNo ratings yet
- Antibiotic Guidelines For BONE AND JOINT INFECTIONSDocument3 pagesAntibiotic Guidelines For BONE AND JOINT INFECTIONSKhurram NadeemNo ratings yet
- Tacar High Resolution Computed Tomography of The LungsDocument79 pagesTacar High Resolution Computed Tomography of The Lungssindy suarezNo ratings yet
- Vidal - Guideline To Successful Worksite Wellness Programs - V1 - 081214Document16 pagesVidal - Guideline To Successful Worksite Wellness Programs - V1 - 081214harihfamNo ratings yet