You might also like
- Pulmonary Tuberculosis Nclex QuestionsDocument3 pagesPulmonary Tuberculosis Nclex Questionssheen100% (7)
- WHO NMH NHD EPG 14.6 EngDocument4 pagesWHO NMH NHD EPG 14.6 EngDr John IfenkweNo ratings yet
- Laboratory Methodologies For Indicators of Iron Status: Strengths, Limitations, and Analytical ChallengesDocument9 pagesLaboratory Methodologies For Indicators of Iron Status: Strengths, Limitations, and Analytical ChallengesudjkwNo ratings yet
- Ferritin Reference Range, Interpretation, Collection and PanelsDocument3 pagesFerritin Reference Range, Interpretation, Collection and Panelson miniNo ratings yet
- Anemia FerropenicaDocument8 pagesAnemia FerropenicaDiego AguilarNo ratings yet
- Iron-Status Indicators: (Miret 2003) (Institute of Medicine 2001)Document16 pagesIron-Status Indicators: (Miret 2003) (Institute of Medicine 2001)Adellia Risda SativaNo ratings yet
- WHO Iron StatusDocument112 pagesWHO Iron StatuskatarinaNo ratings yet
- Ferritin - IMMULITE 2000 Systems - Rev 16 DXDCM 09017fe9802975fc-1538193220913Document33 pagesFerritin - IMMULITE 2000 Systems - Rev 16 DXDCM 09017fe9802975fc-1538193220913ADRIAN MENDOZANo ratings yet
- Níveis de FerroDocument13 pagesNíveis de FerroCarla FernandaNo ratings yet
- Diagnostic Importance of Hepcidin, Soluble TransferrinDocument4 pagesDiagnostic Importance of Hepcidin, Soluble TransferrinushaNo ratings yet
- Iron Metabolism and Its DisordersDocument10 pagesIron Metabolism and Its DisordersMario AbdiwijoyoNo ratings yet
- Serum FerratinDocument4 pagesSerum FerratinSOUMYA A DR, DEPT.OF DENTAL SCIENCES,SRIHERNo ratings yet
- Jurnal Anemia BesiDocument14 pagesJurnal Anemia BesiSonya MaysalvaNo ratings yet
- Serum Transferrin Receptor and Transferrin Receptor-Ferritin Index Identify Healthy Subjects With Subclinical Iron DeficitsDocument6 pagesSerum Transferrin Receptor and Transferrin Receptor-Ferritin Index Identify Healthy Subjects With Subclinical Iron DeficitsekoNo ratings yet
- Camaschella 2017Document9 pagesCamaschella 2017Walter Jhon Delgadillo Arone0% (1)
- Management of Iron de Ficiency: Shuoyan Ning and Michelle P. ZellerDocument8 pagesManagement of Iron de Ficiency: Shuoyan Ning and Michelle P. ZellerGeorgina Aguilar GallardoNo ratings yet
- Health Maintenance II-facultyDocument26 pagesHealth Maintenance II-facultyaliaNo ratings yet
- Haemoglobin Concentrations For The Diagnosis of Anaemia and Assessment of SeverityDocument6 pagesHaemoglobin Concentrations For The Diagnosis of Anaemia and Assessment of Severityniniek yusidaNo ratings yet
- Serum Ferritin and Iron/TIBC of Pregnant Women Attending Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria: A Longitudinal StudyDocument6 pagesSerum Ferritin and Iron/TIBC of Pregnant Women Attending Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria: A Longitudinal StudyasclepiuspdfsNo ratings yet
- WHO - Haemoglobin Level For Anemia 2011Document6 pagesWHO - Haemoglobin Level For Anemia 2011Adhi SanjayaNo ratings yet
- Bohn 2015Document12 pagesBohn 2015katiane.souzaNo ratings yet
- A Short Study On Iron Deficiency in Hostels Using Data Collection FormDocument4 pagesA Short Study On Iron Deficiency in Hostels Using Data Collection FormInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Acta 94 21Document9 pagesActa 94 21ResidenPatKlin Juli2022No ratings yet
- Annex3Document20 pagesAnnex3sitadouk23No ratings yet
- Iron Overload in Beta Thalassemia PDFDocument5 pagesIron Overload in Beta Thalassemia PDFyesikaNo ratings yet
- Iron Deficiency: Review SeriesDocument11 pagesIron Deficiency: Review SeriesWisher PgeNo ratings yet
- 21.iron Deficiency AnemiaDocument10 pages21.iron Deficiency AnemiaArdian SmNo ratings yet
- ArticlesDocument6 pagesArticlesbedahfkumiNo ratings yet
- Monitoring Levels of Iron, TIBC, HB, Transferrin and Ferritin During Pregnancy Trimesters and Lactation in Sulaimania City /iraqDocument3 pagesMonitoring Levels of Iron, TIBC, HB, Transferrin and Ferritin During Pregnancy Trimesters and Lactation in Sulaimania City /iraqMabel StracciaNo ratings yet
- Article 1659164610Document14 pagesArticle 1659164610B49 Nabila Araishabeby YudyatirtaNo ratings yet
- Iron Deficiency AnemiaDocument12 pagesIron Deficiency AnemiaMargarita TorresNo ratings yet
- Annex1 PDFDocument12 pagesAnnex1 PDFTanveerNo ratings yet
- Recommendations To Prevent and Control Iron Deficiency in The United StatesDocument28 pagesRecommendations To Prevent and Control Iron Deficiency in The United StatesAndiFitryanaNo ratings yet
- Iron Balance and The Role of Hepcidin in Chronic Kidney DiseaseDocument11 pagesIron Balance and The Role of Hepcidin in Chronic Kidney DiseaseAdy TaikoNo ratings yet
- Serum Ferritin As An Indicator of Iron Status: What Do We Need To Know?Document6 pagesSerum Ferritin As An Indicator of Iron Status: What Do We Need To Know?udjkwNo ratings yet
- Estimating The Prevalence of Iron Deficiency in The First TwoDocument8 pagesEstimating The Prevalence of Iron Deficiency in The First TwoJavier LunaNo ratings yet
- Deficiencia de Hierro en Falla CardiacaDocument24 pagesDeficiencia de Hierro en Falla CardiacaMarcoNo ratings yet
- Meta Analisis StudiDocument13 pagesMeta Analisis StudiShafira Maulani putriNo ratings yet
- The Relationship Between Depression and Serum Ferritin Level - Shariatpanaahi 2007Document4 pagesThe Relationship Between Depression and Serum Ferritin Level - Shariatpanaahi 2007Julio JuarezNo ratings yet
- 3 - Iron Deficiency Anemia + ACD+Abnormal Heme SynthesisDocument101 pages3 - Iron Deficiency Anemia + ACD+Abnormal Heme SynthesisMotasem ZahaykaNo ratings yet
- Studyprotocol Open AccessDocument9 pagesStudyprotocol Open AccessTeguh SulistiyantoNo ratings yet
- OBGM0291208 EditorialDocument5 pagesOBGM0291208 EditorialRuben SimatupangNo ratings yet
- Special Report Diagnosis and Management of Iron Deficiency in CKD: A Summary of The NICE Guideline Recommendations and Their RationaleDocument11 pagesSpecial Report Diagnosis and Management of Iron Deficiency in CKD: A Summary of The NICE Guideline Recommendations and Their RationaledrnattoNo ratings yet
- Specs 5FE GBDocument5 pagesSpecs 5FE GBkemitaNo ratings yet
- Serum Ferritin - Past, Present and FutureDocument21 pagesSerum Ferritin - Past, Present and FutureAleksandar KitanovskiNo ratings yet
- J1-T5 Anemia FerropénicaDocument12 pagesJ1-T5 Anemia FerropénicaGoblin HunterNo ratings yet
- Ni Hms 590004Document24 pagesNi Hms 590004Muhammad SaqriNo ratings yet
- Iron Chelator DesferrioxamineDocument4 pagesIron Chelator DesferrioxamineMeiyanti MeiyantiNo ratings yet
- Increasing and Decreasing Phases of Ferritin and Hemosiderin Iron Determined by Serum Ferritin KineticsDocument11 pagesIncreasing and Decreasing Phases of Ferritin and Hemosiderin Iron Determined by Serum Ferritin KineticsKaren Flynn HenningNo ratings yet
- Methods Assessment Zinc StatusDocument12 pagesMethods Assessment Zinc Statusmariola.sirventNo ratings yet
- Oral Iron Prophylaxis in Pregnancy Not Too LittleDocument9 pagesOral Iron Prophylaxis in Pregnancy Not Too Littleamit danielNo ratings yet
- Efficacy and Tolerability of Oral Iron Protein Succinylate: A Systematic Review of Three Decades of ResearchDocument12 pagesEfficacy and Tolerability of Oral Iron Protein Succinylate: A Systematic Review of Three Decades of Researchali laftaNo ratings yet
- Assignment 1: Tariq YounasDocument8 pagesAssignment 1: Tariq YounasFT YNo ratings yet
- Ida &da Mini Project EditDocument18 pagesIda &da Mini Project EditAnwesa Priyadarsini PradhanNo ratings yet
- Body Iron StoreDocument20 pagesBody Iron StoreAnonymous vmMUoBnNo ratings yet
- Dr. Palwasha Hayat Burki PG Trainee (Paeds)Document104 pagesDr. Palwasha Hayat Burki PG Trainee (Paeds)Saba WaheedNo ratings yet
- Food-Based Approaches For Combating Iron Deficiency: Food and Agriculture Organization (FAO), Rome, ItalyDocument23 pagesFood-Based Approaches For Combating Iron Deficiency: Food and Agriculture Organization (FAO), Rome, ItalyEnik guntyastutikNo ratings yet
- Iron Status and Choice of Iron Therapy During Pregnancy: Advantages and DisadvantagesDocument8 pagesIron Status and Choice of Iron Therapy During Pregnancy: Advantages and DisadvantagesTenri Syahira SaidNo ratings yet
- Research Article: Ferritin Is A Marker of Inflammation Rather Than Iron Deficiency in Overweight and Obese PeopleDocument8 pagesResearch Article: Ferritin Is A Marker of Inflammation Rather Than Iron Deficiency in Overweight and Obese PeopleTanveerNo ratings yet
- Iron therapy - With Special Emphasis on Intravenous AdministrationFrom EverandIron therapy - With Special Emphasis on Intravenous AdministrationNo ratings yet
- Dry Needling Article PMRDocument8 pagesDry Needling Article PMRRo KohnNo ratings yet
- Dentsply The Difference Edition 4Document24 pagesDentsply The Difference Edition 4AD TwentyOne DentalNo ratings yet
- Nursing As A ProfessionDocument164 pagesNursing As A ProfessionLex Alejandro Jr.No ratings yet
- Kartu StokDocument22 pagesKartu Stokputri purnamasariNo ratings yet
- Drug StudyDocument19 pagesDrug StudyCalimlim KimNo ratings yet
- Case Study Hypertension 1Document11 pagesCase Study Hypertension 1Irwan 'Iw Iw' Setiawan100% (2)
- UP PGH Department of Surgery 52nd Post Graduate Course: Oncologic Surgery Current Concepts and ManagementDocument74 pagesUP PGH Department of Surgery 52nd Post Graduate Course: Oncologic Surgery Current Concepts and ManagementAceAlfabeto100% (3)
- GangreneDocument6 pagesGangreneMohammad Yordan GandaraNo ratings yet
- Short Reports: Amiodarone Increases Plasma Digoxin ConcentrationsDocument1 pageShort Reports: Amiodarone Increases Plasma Digoxin Concentrationseki_megaraniNo ratings yet
- 8 Abnormal BehaviorDocument34 pages8 Abnormal BehaviorRyanito MarquezNo ratings yet
- Lecture Slides On The Theories On Counseling (Existential and Gestalt)Document34 pagesLecture Slides On The Theories On Counseling (Existential and Gestalt)Norton100% (2)
- Speech & Language Therapy in Practice, Winter 2010Document36 pagesSpeech & Language Therapy in Practice, Winter 2010Speech & Language Therapy in PracticeNo ratings yet
- Buka J of Cosmetic Dermatology - 2022 - Arora - Cellulite Presentation and Management PDFDocument9 pagesBuka J of Cosmetic Dermatology - 2022 - Arora - Cellulite Presentation and Management PDFMamakNya VidyaNo ratings yet
- Steroid Vs Splint in CtsDocument11 pagesSteroid Vs Splint in CtsDiayanti TentiNo ratings yet
- MCQDocument5 pagesMCQJagdishVankar100% (2)
- Parental Presence Vs Absence - Dr. Julie ManiateDocument27 pagesParental Presence Vs Absence - Dr. Julie ManiateRooka82No ratings yet
- Biopharmaceutics Supplemental NotesDocument19 pagesBiopharmaceutics Supplemental NotesChristine Joy De Ocampo0% (1)
- Alcoholic Liver DiseaseDocument3 pagesAlcoholic Liver DiseaseEglNo ratings yet
- Week 7 - Rheumatoid ArthritisDocument1 pageWeek 7 - Rheumatoid ArthritisTuTitNo ratings yet
- Psychosocial Approaches in Schizophrenia: Presenter: Dr.D.Archanaa Chairperson: Ms - NeethiDocument61 pagesPsychosocial Approaches in Schizophrenia: Presenter: Dr.D.Archanaa Chairperson: Ms - NeethidarchanaavigneshNo ratings yet
- Isabelle Kiritsy Master ResumeDocument2 pagesIsabelle Kiritsy Master Resumeapi-355753645No ratings yet
- Implant PanaceaDocument2 pagesImplant PanaceaKarina OjedaNo ratings yet
- Alvin Gabriel L. AltarejosDocument17 pagesAlvin Gabriel L. AltarejosKeanu AlvarezNo ratings yet
- Children With Special NeedsDocument18 pagesChildren With Special NeedsNmm Safeek25% (4)
- S Tahel 2005Document12 pagesS Tahel 2005Catherine MorrisNo ratings yet
- URAPIDILDocument41 pagesURAPIDILFrancesco LucianiNo ratings yet
- AyurvedaDocument15 pagesAyurvedaisce5b100% (1)
- Group DynamicsDocument21 pagesGroup DynamicsDeena Melvin100% (3)
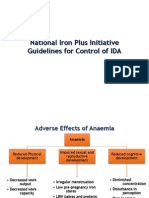
- National Iron Plus Initiative Guidelines For Controlof IDADocument19 pagesNational Iron Plus Initiative Guidelines For Controlof IDAvvirumbi100% (1)