You might also like
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- CPPT IN THE ICUDocument39 pagesCPPT IN THE ICUeyob kaseyeNo ratings yet
- Management of Critically Ill Patients in The ICUDocument55 pagesManagement of Critically Ill Patients in The ICUkader abdiNo ratings yet
- Anesthesia techniques for cardiac surgeryDocument179 pagesAnesthesia techniques for cardiac surgerymd.dascalescu2486No ratings yet
- Basics of AnesthesiaDocument34 pagesBasics of Anesthesianicolinna2000yahoo.comNo ratings yet
- Principles of CPR and CARDIAC MASSAGEDocument34 pagesPrinciples of CPR and CARDIAC MASSAGEBharat BhushanNo ratings yet
- Theme 1 1Document97 pagesTheme 1 1lela ndociNo ratings yet
- Cardiac SurgeryDocument19 pagesCardiac SurgerySimon JosanNo ratings yet
- Surgical Critical Care ReviewDocument70 pagesSurgical Critical Care ReviewSteven GodelmanNo ratings yet
- Cardiac Cath and Monitoring ProceduresDocument40 pagesCardiac Cath and Monitoring ProceduresMarissa AsimNo ratings yet
- An Introduction To Surgical Icu.: by DR Farrukh SaeedDocument33 pagesAn Introduction To Surgical Icu.: by DR Farrukh SaeedTARIQNo ratings yet
- 1095 Preoperative Risk Stratification and OptimizationDocument99 pages1095 Preoperative Risk Stratification and OptimizationHening Tirta KusumawardaniNo ratings yet
- Jason Wolfe's ATLS Trauma Moulage Page: (Thoughts On The Management of The Multiply Injured Patient)Document18 pagesJason Wolfe's ATLS Trauma Moulage Page: (Thoughts On The Management of The Multiply Injured Patient)gogopal100% (6)
- Oxygen Therapy GuideDocument12 pagesOxygen Therapy Guideأحمد أسامهNo ratings yet
- Chapter 5 Cardiovascular EmergenciesDocument6 pagesChapter 5 Cardiovascular Emergenciesعلاء البناءNo ratings yet
- Cabg 130102113345 Phpapp01Document29 pagesCabg 130102113345 Phpapp01md.dascalescu2486No ratings yet
- ACLS Pulmonary Edema and Stroke AlgorithmsDocument34 pagesACLS Pulmonary Edema and Stroke AlgorithmsMuhammad SafaatNo ratings yet
- Special Resuscitation Situations: Stroke, Hypothermia, Anaphylaxis, Drowning, Trauma, PregnancyDocument55 pagesSpecial Resuscitation Situations: Stroke, Hypothermia, Anaphylaxis, Drowning, Trauma, PregnancyPrincess Cate MercadoNo ratings yet
- Emed - Special Resuscitation Situations (Doc Vito)Document55 pagesEmed - Special Resuscitation Situations (Doc Vito)Princess Cate MercadoNo ratings yet
- CCPACatheter Basics 07 MedicineDocument44 pagesCCPACatheter Basics 07 MedicinerinbijoyNo ratings yet
- Core ACLS ConceptsDocument60 pagesCore ACLS ConceptsLex CatNo ratings yet
- Nelec2 Week 17Document13 pagesNelec2 Week 17Michelle MallareNo ratings yet
- Week 5 Respiratory EmergencyDocument61 pagesWeek 5 Respiratory EmergencyArmand Bong SantiagoNo ratings yet
- 8 - DR. Khaled - Cardiac SurgeryDocument26 pages8 - DR. Khaled - Cardiac SurgeryMuhand.No ratings yet
- Hemodynamic MonitoringDocument4 pagesHemodynamic Monitoringgurneet kourNo ratings yet
- Pre Operative AssessmentDocument33 pagesPre Operative AssessmentShimmering MoonNo ratings yet
- Acls 30-10-23Document63 pagesAcls 30-10-23lakshmiNo ratings yet
- Cardiac Arrest - BLS-ACLS - Dr. KhaledDocument93 pagesCardiac Arrest - BLS-ACLS - Dr. Khaledrony ghoshNo ratings yet
- Artery Bypass GraftDocument3 pagesArtery Bypass GraftJasmine ChuaNo ratings yet
- Echocerdiografi EmergencyDocument45 pagesEchocerdiografi EmergencyRiska ViandiniNo ratings yet
- Ramilo, Sheena Patricia M. Ncenh06Document4 pagesRamilo, Sheena Patricia M. Ncenh06JaysellePuguonTabijeNo ratings yet
- Transportation and Stabilitation in Critically Ill Patient - 2015Document36 pagesTransportation and Stabilitation in Critically Ill Patient - 2015Gustav Valentino100% (1)
- Post-Cardiac Arrest CareDocument16 pagesPost-Cardiac Arrest CareJeremia KurniawanNo ratings yet
- Model Answer -I & II سبتمبر 2015تحريريDocument12 pagesModel Answer -I & II سبتمبر 2015تحريريAmr El TaherNo ratings yet
- Hemodynamic MonitoringDocument46 pagesHemodynamic MonitoringSonia khanNo ratings yet
- CPR 2014 SeminarDocument43 pagesCPR 2014 SeminarMinale MenberuNo ratings yet
- 2 Understanding ICU EquipmentDocument45 pages2 Understanding ICU EquipmentAbhinav DuttaNo ratings yet
- Perioperative Evaluation: Dr. Deasiana Paksi Moeda SP.B, Finacs 24 Agustus 2021Document30 pagesPerioperative Evaluation: Dr. Deasiana Paksi Moeda SP.B, Finacs 24 Agustus 2021ZaniaNo ratings yet
- Cardiac ArrestDocument40 pagesCardiac ArrestApriliani Nur Puspita SariNo ratings yet
- Basics of AnesthesiaDocument34 pagesBasics of Anesthesiadremad1974No ratings yet
- Crash CartDocument3 pagesCrash CartRasheila Palti RNNo ratings yet
- Cardiology NotesDocument13 pagesCardiology NotesFreeNursingNotes78% (9)
- Tetralogy of FallotDocument41 pagesTetralogy of Fallotthecount28991No ratings yet
- Advanced Cardiac Life SupportDocument42 pagesAdvanced Cardiac Life SupportDennis MiritiNo ratings yet
- Lung Expansion RevisionDocument89 pagesLung Expansion RevisionPatrick RoqueNo ratings yet
- CPR EffectivenessDocument68 pagesCPR EffectivenessKIMS qualityNo ratings yet
- 3730 Monitoring Hemodinamik-2019Document52 pages3730 Monitoring Hemodinamik-2019ojika olandaNo ratings yet
- ACLSDocument61 pagesACLSmgthida935100% (1)
- Open Heart 1Document18 pagesOpen Heart 1mohamedNo ratings yet
- Monitoring PerioperatipDocument54 pagesMonitoring Perioperatipjavajavu100% (1)
- Physiologic Basis Hemodynamic MonitoringDocument36 pagesPhysiologic Basis Hemodynamic MonitoringEshwar Chandra VidyasagarNo ratings yet
- Cardioplumonary RDocument40 pagesCardioplumonary RABREHAM BUKULONo ratings yet
- Cardiac Content WyattDocument90 pagesCardiac Content WyattAnni BarbaNo ratings yet
- Role of Physiotherapy in ICUDocument68 pagesRole of Physiotherapy in ICUprasanna3k100% (2)
- AtlsDocument23 pagesAtlsvivi chanNo ratings yet
- Medical Emergency Oral Q.docx26.docx8Document44 pagesMedical Emergency Oral Q.docx26.docx8Simina ÎntunericNo ratings yet
- Case Study - Cardio FunctionDocument3 pagesCase Study - Cardio FunctionJrBong Semanero100% (1)
- Procedural AnesthesiaDocument40 pagesProcedural AnesthesiaJovian LutfiNo ratings yet
- Acute HF-IAIDocument49 pagesAcute HF-IAIAndita ListyannisaNo ratings yet
- Course Topic Cu11 DigestionDocument14 pagesCourse Topic Cu11 DigestionMichelle MallareNo ratings yet
- Nelec2 Week 17Document13 pagesNelec2 Week 17Michelle MallareNo ratings yet
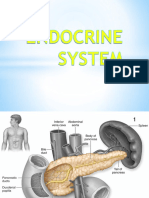
- EndocrineDocument32 pagesEndocrineMichelle MallareNo ratings yet
- Critical Care Nursing: Bachelor of Science in NursingDocument4 pagesCritical Care Nursing: Bachelor of Science in NursingMichelle MallareNo ratings yet
- Nursing Informatics: Bachelor of Science in NursingDocument5 pagesNursing Informatics: Bachelor of Science in NursingMichelle MallareNo ratings yet
- OBCL 1 - WEEK 13 ELIMINATION (Course Module)Document15 pagesOBCL 1 - WEEK 13 ELIMINATION (Course Module)Michelle MallareNo ratings yet
- Abc M3 Cu11Document4 pagesAbc M3 Cu11Michelle MallareNo ratings yet
- Spinal Cord InjuryDocument23 pagesSpinal Cord InjuryMichelle MallareNo ratings yet
- Course Topic Cu11 DigestionDocument14 pagesCourse Topic Cu11 DigestionMichelle MallareNo ratings yet
- Obcl 1 Week 10 CirculationDocument23 pagesObcl 1 Week 10 CirculationMichelle MallareNo ratings yet
- Essential Communication Skills for NursingDocument31 pagesEssential Communication Skills for NursingMichelle MallareNo ratings yet
- Obcl 1 Week 16 Perception and CoordinationDocument20 pagesObcl 1 Week 16 Perception and CoordinationMichelle Mallare100% (1)
- Obcl 1 Week 16 Perception and CoordinationDocument20 pagesObcl 1 Week 16 Perception and CoordinationMichelle Mallare100% (1)
- Integumentary System: Vilma R. Miguel, MAN, RNDocument117 pagesIntegumentary System: Vilma R. Miguel, MAN, RNMichelle MallareNo ratings yet
- Care of Clients With Cellular Aberrations: Bachelor of Science in NursingDocument4 pagesCare of Clients With Cellular Aberrations: Bachelor of Science in NursingMichelle MallareNo ratings yet
- ECGDocument118 pagesECGMichelle MallareNo ratings yet
- Acute Renal Failure Nursing Care and ManagementDocument7 pagesAcute Renal Failure Nursing Care and ManagementMichelle MallareNo ratings yet
- Critical Care Nursing: Airway Obstruction ManagementDocument8 pagesCritical Care Nursing: Airway Obstruction ManagementMichelle MallareNo ratings yet
- Breast Case AnalysisDocument5 pagesBreast Case AnalysisMichelle MallareNo ratings yet
- Course Topic-Obcl 1cm1-Cu5Document19 pagesCourse Topic-Obcl 1cm1-Cu5Michelle MallareNo ratings yet
- Ilovepdf MergedDocument10 pagesIlovepdf MergedMichelle MallareNo ratings yet
- Small Group CommunicationDocument10 pagesSmall Group CommunicationMichelle MallareNo ratings yet
- Nelec2 Week 7Document11 pagesNelec2 Week 7Michelle MallareNo ratings yet
- Bachelor of Science in Nursing: NCM 106 Skills Laboratory: Laboratory Module Laboratory Unit WeekDocument6 pagesBachelor of Science in Nursing: NCM 106 Skills Laboratory: Laboratory Module Laboratory Unit WeekMichelle MallareNo ratings yet
- Nelec2 Week 9Document6 pagesNelec2 Week 9Michelle MallareNo ratings yet
- N106 Week9Document3 pagesN106 Week9Michelle MallareNo ratings yet
- Nelec2 Week 10Document8 pagesNelec2 Week 10Michelle MallareNo ratings yet
- Nelec2 Week 11Document9 pagesNelec2 Week 11Michelle MallareNo ratings yet
- Nursing Informatics: Bachelor of Science in NursingDocument4 pagesNursing Informatics: Bachelor of Science in NursingMichelle MallareNo ratings yet
- Specialty Doctor ICU & Anaesthetics RoleDocument20 pagesSpecialty Doctor ICU & Anaesthetics RolejahangirealamNo ratings yet
- Anaesthesia Syllabus BfuhsDocument22 pagesAnaesthesia Syllabus BfuhsHarshit ChempallilNo ratings yet
- Management Sepsis TerkiniDocument82 pagesManagement Sepsis TerkiniSyahrul HamidNo ratings yet
- Evaluation of An Advanced Practice Provider Emergency Department Critical Care Step-Down UnitDocument11 pagesEvaluation of An Advanced Practice Provider Emergency Department Critical Care Step-Down UnitMiva MaviniNo ratings yet
- Electronic Patient Record Use During Ward Rounds: A Qualitative Study of Interaction Between Medical StaffDocument8 pagesElectronic Patient Record Use During Ward Rounds: A Qualitative Study of Interaction Between Medical StaffpsikubNo ratings yet
- Conference Reports and Expert Panel: DOI 10.1007/s00134-017-4919-5Document13 pagesConference Reports and Expert Panel: DOI 10.1007/s00134-017-4919-5Mari ArcenganNo ratings yet
- Training Programs in LCPDocument6 pagesTraining Programs in LCPHarbyNo ratings yet
- Rekap Barang Alat Medis RSU ProklamasiDocument10 pagesRekap Barang Alat Medis RSU ProklamasiSandi PrawiranegaraNo ratings yet
- Action ResearchDocument12 pagesAction ResearchLee CelNo ratings yet
- Critical Appraisal Nurse Staffing and Inpatient Hospital MortalityDocument42 pagesCritical Appraisal Nurse Staffing and Inpatient Hospital Mortalitykristina dewiNo ratings yet
- Esicm 2020Document612 pagesEsicm 2020FERNANDODEJESUS LOPEZ RUEDANo ratings yet
- Rsud Konawe SelatanDocument6 pagesRsud Konawe SelatanewNo ratings yet
- Nursing Leadership Analysis PaperDocument9 pagesNursing Leadership Analysis Paperapi-240099055100% (2)
- Intermediate Care Unit - An Efficient and Flexible Facility, or A "Limbo" Between ICU and Ward?Document3 pagesIntermediate Care Unit - An Efficient and Flexible Facility, or A "Limbo" Between ICU and Ward?JHNo ratings yet
- Viewpoint: Claudio Ronco, Thiago Reis, Faeq Husain-SyedDocument5 pagesViewpoint: Claudio Ronco, Thiago Reis, Faeq Husain-SyedAbdul RahimNo ratings yet
- VeterinaryDocument21 pagesVeterinaryuse19777851100% (3)
- Burnout SyndromeDocument2 pagesBurnout SyndromeAlina NeagoeNo ratings yet
- Arterial Blood Gas (ABG) AnalysisDocument37 pagesArterial Blood Gas (ABG) AnalysisronDITCHvon SalindoNo ratings yet
- DR Mohammed Azam Danish CVDocument1 pageDR Mohammed Azam Danish CVthat savage guyNo ratings yet
- Brief History of VL Makabali Memorial HospitalDocument1 pageBrief History of VL Makabali Memorial Hospitalpaulo_070390100% (1)
- CGHS Empanelled Hospitals in BangaloreDocument15 pagesCGHS Empanelled Hospitals in BangaloreJust ChemicalsNo ratings yet
- Religare Care Insurance Policy WordingDocument13 pagesReligare Care Insurance Policy WordingShakti ShivanandNo ratings yet
- Clinical ExemplarDocument4 pagesClinical Exemplarapi-608069746No ratings yet
- The Effects of Environmental Stressors in Intensive Care Unit Onanxiety and DepressionDocument7 pagesThe Effects of Environmental Stressors in Intensive Care Unit Onanxiety and DepressionAyda KebapçıNo ratings yet
- Acid-Base Imbalances: Dr. Emmanuel Sandy Department of Chemical Pathology Comahs-UslDocument49 pagesAcid-Base Imbalances: Dr. Emmanuel Sandy Department of Chemical Pathology Comahs-UslVivian KamaraNo ratings yet
- Critical Care Nursing Role in Patient MonitoringDocument2 pagesCritical Care Nursing Role in Patient Monitoringkarl montano100% (1)
- Registered Nurse with 13 Years of ER ExperienceDocument2 pagesRegistered Nurse with 13 Years of ER ExperienceDina TrisnawatiNo ratings yet
- Clinical Scenarios in ICUDocument107 pagesClinical Scenarios in ICUmatenten100% (4)
- The Honourable Jason CoppingDocument3 pagesThe Honourable Jason Coppingedmontonjournal100% (1)
- Project Proposal: Code of 1991 Mandates The Local Government Units To Provide Basic FacilitiesDocument4 pagesProject Proposal: Code of 1991 Mandates The Local Government Units To Provide Basic Facilitiescasagantm-1No ratings yet