You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- DryDock CompleteDocument24 pagesDryDock Completeashry_tarek100% (2)
- Walking The Talk Duponts Untold Safety FailuresDocument28 pagesWalking The Talk Duponts Untold Safety Failuressl1828No ratings yet
- Glenn B. Gagante, Emt, Ert, Smrismgt: EskwelDocument12 pagesGlenn B. Gagante, Emt, Ert, Smrismgt: EskwelAna Rose M. LlameraNo ratings yet
- FRM Part 2 - Practice Book - Volume 2 - 2021Document146 pagesFRM Part 2 - Practice Book - Volume 2 - 2021Mridul Saraf100% (1)
- Sean Messenger Blog ExtractDocument74 pagesSean Messenger Blog Extractruffin100No ratings yet
- Virtual Certified Supplier Quality ProfessionalDocument1 pageVirtual Certified Supplier Quality ProfessionalPapaiNo ratings yet
- Aqa A2 Biology LDRDocument21 pagesAqa A2 Biology LDRjames100% (4)
- API Standard Storage Tank Data Sheet Rev 0Document3 pagesAPI Standard Storage Tank Data Sheet Rev 0Ari HidayatNo ratings yet
- Eddy Current Testing in NDTDocument43 pagesEddy Current Testing in NDTMeby Selvaraj RNo ratings yet
- Peoples Pharmacy Job ApplicationDocument2 pagesPeoples Pharmacy Job ApplicationNoushin ShaikNo ratings yet
- PeoplesPharmacyJobApplication Update2020Document2 pagesPeoplesPharmacyJobApplication Update2020Noushin ShaikNo ratings yet
- DH Fire Training Schedule Jan 26-29, 2021Document15 pagesDH Fire Training Schedule Jan 26-29, 2021Noushin ShaikNo ratings yet
- British Virgin IslandsDocument2 pagesBritish Virgin IslandsNoushin ShaikNo ratings yet
- November 2018 (9-1) MS - Paper 3 CIE Biology IGCSEDocument12 pagesNovember 2018 (9-1) MS - Paper 3 CIE Biology IGCSEmahanetsarapelang64No ratings yet
- Sika Anchorfix®-2+ Tropical: Product Data SheetDocument5 pagesSika Anchorfix®-2+ Tropical: Product Data SheetM. KumaranNo ratings yet
- Exercise 2Document9 pagesExercise 2Meryem LamhamdiNo ratings yet
- Stuffed PeppersDocument2 pagesStuffed PeppersDewayne AginNo ratings yet
- MasterFlow An Brochure FinalDocument12 pagesMasterFlow An Brochure FinalNavinNo ratings yet
- CEA & Hostel SubsidyDocument8 pagesCEA & Hostel SubsidySakib ShaikhNo ratings yet
- 11.8 Chemical Equilibrium Solution - PremiumDocument20 pages11.8 Chemical Equilibrium Solution - PremiumJonathan ParkerNo ratings yet
- Services Bulletins Model 150kDocument8 pagesServices Bulletins Model 150kPaola RabeloNo ratings yet
- Drug StudyDocument9 pagesDrug StudyPantaleon PacisNo ratings yet
- Distribution of School Supplies NamesDocument16 pagesDistribution of School Supplies Namesdyesabel LibresNo ratings yet
- Answers For Practice Problems in Lesson 5: Practice Problem #1: Specific Gravity Calculation For Coarse AggregateDocument2 pagesAnswers For Practice Problems in Lesson 5: Practice Problem #1: Specific Gravity Calculation For Coarse AggregateDjonraeNarioGalvezNo ratings yet
- 2010 Pulse Processing Functionality and Application Litera.Document145 pages2010 Pulse Processing Functionality and Application Litera.abid222No ratings yet
- WinS Monitoring System - Blank v2017!06!04Document17 pagesWinS Monitoring System - Blank v2017!06!04Sab Caramol Dael80% (5)
- Swedish Neutral Neutral Earthing Resistor Specification PDFDocument12 pagesSwedish Neutral Neutral Earthing Resistor Specification PDFRazvan CostacheNo ratings yet
- ! 19 Organic Rankine CycleDocument14 pages! 19 Organic Rankine Cyclesapcuta16smenNo ratings yet
- Anatomi BBB: Hilmi Adyatma 1710211069Document13 pagesAnatomi BBB: Hilmi Adyatma 1710211069Hilmi AdyatmaNo ratings yet
- Final SPMCWaiverfortraineesandaffiliatesDocument3 pagesFinal SPMCWaiverfortraineesandaffiliatesSuzanne AndresNo ratings yet
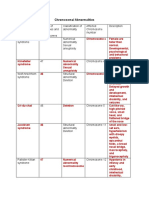
- Table On Chromosomal AbnormalitiesDocument3 pagesTable On Chromosomal AbnormalitiesJoanne Mary RomoNo ratings yet
- Promotion of Liquor in GujaratDocument17 pagesPromotion of Liquor in Gujaratrakesh_jain86No ratings yet
- Cat Fines Guidance PDFDocument4 pagesCat Fines Guidance PDFStefas DimitriosNo ratings yet
- DS-Vitopelx 200-Type SX2A - 5728770 - 6 - VDPDocument14 pagesDS-Vitopelx 200-Type SX2A - 5728770 - 6 - VDPDamir MuslicNo ratings yet