You might also like
- Construction of Labial Bow.: June 2012Document2 pagesConstruction of Labial Bow.: June 2012lauraNo ratings yet
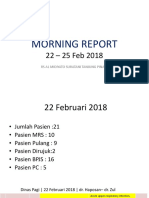
- MR 22-25 Feb FIXED (Autosaved)Document21 pagesMR 22-25 Feb FIXED (Autosaved)lauraNo ratings yet
- Dinas Siang - 5 Februari 2018 - Dr. Bambang - Dr. Raja: SebetulDocument2 pagesDinas Siang - 5 Februari 2018 - Dr. Bambang - Dr. Raja: SebetullauraNo ratings yet
- Death Case PPT Blum JDDocument15 pagesDeath Case PPT Blum JDlauraNo ratings yet
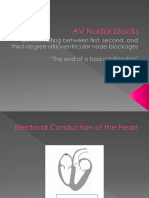
- AV Nodal BlocksDocument13 pagesAV Nodal BlockslauraNo ratings yet
- Sick Sinus SyndromeDocument12 pagesSick Sinus Syndromelaura100% (1)
- Morning Report 22-25 FebDocument21 pagesMorning Report 22-25 FeblauraNo ratings yet
- Morning Report: Rs Al Midiyato Suratani Tanjung PinangDocument16 pagesMorning Report: Rs Al Midiyato Suratani Tanjung PinanglauraNo ratings yet
- Morning Report Raja (Autosaved)Document1 pageMorning Report Raja (Autosaved)lauraNo ratings yet
- Febris, Unspecified Febris, Unspecified: Non Traumatic, Intraventricular HemorrhageDocument1 pageFebris, Unspecified Febris, Unspecified: Non Traumatic, Intraventricular HemorrhagelauraNo ratings yet
- Dinas Pagi - 22 Februari 2018 - Dr. Haposan - Dr. RajaDocument4 pagesDinas Pagi - 22 Februari 2018 - Dr. Haposan - Dr. RajalauraNo ratings yet
- Sylla Fitria Wardany Abu Bakar Medan, 25 Oktober 2006Document1 pageSylla Fitria Wardany Abu Bakar Medan, 25 Oktober 2006lauraNo ratings yet
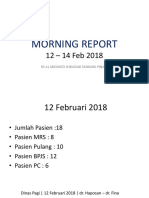
- Morning Report 01-04 2018Document4 pagesMorning Report 01-04 2018lauraNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Đáp Án Trung Học Thực Hành Đại Học Sư Phạm 2020-2021Document12 pagesĐáp Án Trung Học Thực Hành Đại Học Sư Phạm 2020-2021Chi Vũ LinhNo ratings yet
- Investigation of An Animal Mutilation Injuries in Cache County, UtahDocument33 pagesInvestigation of An Animal Mutilation Injuries in Cache County, UtahLionel Elyansun100% (1)
- Microwave Diathermy: Physiotherapy Treatment ModalitiesDocument7 pagesMicrowave Diathermy: Physiotherapy Treatment ModalitiesKids LearningcenterNo ratings yet
- Lázár Et Al. - 2018 - Collateral Sensitivity To Antimicrobial Peptides - Nature Microbiology PDFDocument17 pagesLázár Et Al. - 2018 - Collateral Sensitivity To Antimicrobial Peptides - Nature Microbiology PDFYago QSNo ratings yet
- Proposed Child Right's Policy FrameworkDocument2 pagesProposed Child Right's Policy FrameworkCrisDBNo ratings yet
- VELANKANNI Tourist GuideDocument12 pagesVELANKANNI Tourist Guideshiva1720No ratings yet
- Adult Use DispensariesDocument8 pagesAdult Use DispensariesRomeeNo ratings yet
- AviPro News Issue 4Document8 pagesAviPro News Issue 4Bryan NicollNo ratings yet
- RA 7876 Senior Citizen CenterDocument3 pagesRA 7876 Senior Citizen CenterreadretainunderstandNo ratings yet
- Infant and Child Nutrition: Key PointsDocument4 pagesInfant and Child Nutrition: Key PointsseptiNo ratings yet
- Taski D7 Msds - Free PDFDocument3 pagesTaski D7 Msds - Free PDFanushkasamantha0% (1)
- Power of 16 MahaVastu™ Zones Vastu Remedy 3Document1 pagePower of 16 MahaVastu™ Zones Vastu Remedy 3ritikNo ratings yet
- Manual de Instalación - Aures-Slim-Multi - AristonDocument82 pagesManual de Instalación - Aures-Slim-Multi - Aristonoscar.diaz.joveNo ratings yet
- Stok 14.12.2022 SalesmanDocument8 pagesStok 14.12.2022 Salesmanrusnansyah unanNo ratings yet
- Process RecordingDocument4 pagesProcess RecordingAnnette Aquino GuevarraNo ratings yet
- STS Module 12 Biodiversity and The Healthy Society EnhancedDocument44 pagesSTS Module 12 Biodiversity and The Healthy Society EnhancedRyan Fernandez Dela CruzNo ratings yet
- Letter - Mayor Johnson - 20181207Document2 pagesLetter - Mayor Johnson - 20181207Alyssa RobertsNo ratings yet
- List BibliographyDocument10 pagesList BibliographyFabian BarretoNo ratings yet
- PICS-AICS AP 2015 - Poster Presentation ListDocument2 pagesPICS-AICS AP 2015 - Poster Presentation ListDian Asri ChenelNo ratings yet
- Stakeholders Engagement Plan - EJREDocument21 pagesStakeholders Engagement Plan - EJREVikrant PathaniaNo ratings yet
- Esic List of Holiday HomesDocument7 pagesEsic List of Holiday HomesUday Amar100% (1)
- NutritionDocument3 pagesNutritionDinesh Kumar0% (5)
- Acute Vestibular Syndrome: David E. Newman-Toker, MD, PHDDocument0 pagesAcute Vestibular Syndrome: David E. Newman-Toker, MD, PHDArturo CeraciNo ratings yet
- Nate Resume NoinfoDocument2 pagesNate Resume Noinfoapi-244170629No ratings yet
- Coa CfuDocument18 pagesCoa CfuZymer Lee AbasoloNo ratings yet
- Geriatric Depression ScaleDocument2 pagesGeriatric Depression ScaleBadru SuhufNo ratings yet
- Massage Intake and Agreement Form CoreDocument2 pagesMassage Intake and Agreement Form CoreCraig JohnsonNo ratings yet
- Roland Berger - Pharmaceutical Industry Study 2009 - What Is NextDocument40 pagesRoland Berger - Pharmaceutical Industry Study 2009 - What Is Nextapritul3539No ratings yet
- Bill de Blasio - One New York Rising TogetherDocument75 pagesBill de Blasio - One New York Rising TogetherStefano AmbrosiniNo ratings yet
- ISPE Presentation Water Steam Systems 1681853503Document69 pagesISPE Presentation Water Steam Systems 1681853503brunojp83No ratings yet