You might also like
- Rehab Cheat SheetDocument18 pagesRehab Cheat SheetZ A100% (3)
- Medical Certificate for Cough, Sore Throat, HeadacheDocument1 pageMedical Certificate for Cough, Sore Throat, HeadacheJareena SamsonNo ratings yet
- Case HistoryDocument12 pagesCase HistoryEmmanuel Rojith Vaz0% (1)
- Eyelid Anatomy and Common Disorders GuideDocument26 pagesEyelid Anatomy and Common Disorders Guideking darkNo ratings yet
- Escoton, Kate Angel P (NCP)Document4 pagesEscoton, Kate Angel P (NCP)Kate EscotonNo ratings yet
- Bukidnon State University College of NursingDocument5 pagesBukidnon State University College of NursingAIZA MAE BANGGAY100% (1)
- Pain AssessmntDocument2 pagesPain Assessmntmohs2007100% (1)
- Medical Surgical NursingDocument59 pagesMedical Surgical Nursingnot your medz duranNo ratings yet
- Medical Surgical NursingDocument66 pagesMedical Surgical Nursing04eden100% (3)
- Andrian Dwi Herlambang (P17230181001) Acute PainDocument8 pagesAndrian Dwi Herlambang (P17230181001) Acute PainAndrian TakigawaNo ratings yet
- NCP PainDocument4 pagesNCP PainFlauros Ryu JabienNo ratings yet
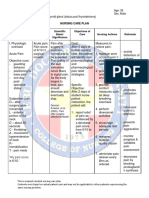
- Problem Scientific Basis Goals/Objectives Criteria Nursing Interventions Rationale Evaluation Date: November 9, 2021 Time: 10:00 AM Nursing Diagnosis: Goal Partially METDocument2 pagesProblem Scientific Basis Goals/Objectives Criteria Nursing Interventions Rationale Evaluation Date: November 9, 2021 Time: 10:00 AM Nursing Diagnosis: Goal Partially METGwyneth Christine TanNo ratings yet
- Typhoid Fever NCPDocument46 pagesTyphoid Fever NCPLyra Lustre RN67% (3)
- Nursing Care PlanDocument19 pagesNursing Care Planabigail gogoNo ratings yet
- Assessment NyeriDocument18 pagesAssessment NyerisnookumsnjNo ratings yet
- Nursing Care for Acute PainDocument3 pagesNursing Care for Acute PainJared Niles SantosNo ratings yet
- Diagnostic Findings:: Short Term Goal Short Term GoalDocument3 pagesDiagnostic Findings:: Short Term Goal Short Term GoalGiselle EstoquiaNo ratings yet
- Finals Notes UnfinishedDocument23 pagesFinals Notes UnfinishedNicholeGarcesCisnerosNo ratings yet
- College Nursing Care Plan TemplateDocument9 pagesCollege Nursing Care Plan TemplateCecil MonteroNo ratings yet
- Appendicitis - NCPDocument5 pagesAppendicitis - NCPEarl Joseph Deza100% (1)
- Appendicitis NCPDocument5 pagesAppendicitis NCPEarl Joseph DezaNo ratings yet
- Prioritizing Nursing Problems and Interventions for Postpartum PainDocument2 pagesPrioritizing Nursing Problems and Interventions for Postpartum PainFia GregorioNo ratings yet
- Idc NCPDocument14 pagesIdc NCPEnrique BabierraNo ratings yet
- Module 2M: Concept of PainDocument3 pagesModule 2M: Concept of PainDominic DegraciaNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainGeorge FogNo ratings yet
- Pain and Fever (Reviewer)Document5 pagesPain and Fever (Reviewer)James Lord GalangNo ratings yet
- Updated CH 30 Pain Assessment and ManagementDocument30 pagesUpdated CH 30 Pain Assessment and Managementaabbccss1.z71No ratings yet
- Nursing Care Plan: Western Mindanao State University College of NursingDocument11 pagesNursing Care Plan: Western Mindanao State University College of NursingPatricia VasquezNo ratings yet
- Actual NCPDocument10 pagesActual NCPRouie Björn ABrianNo ratings yet
- NCM117 NCPDocument2 pagesNCM117 NCPHANNAH MICOLE GAERLANNo ratings yet
- Post-Operative Nursing Care Plan # 1Document14 pagesPost-Operative Nursing Care Plan # 1Vince John SevillaNo ratings yet
- Nursing Care Plan for Post-Surgical Pain ManagementDocument7 pagesNursing Care Plan for Post-Surgical Pain ManagementMacris BondocNo ratings yet
- 5 Hamad Core Comeptencies FinalDocument2 pages5 Hamad Core Comeptencies FinalvhonNo ratings yet
- PainDocument2 pagesPainAshley TwinkleNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanRohmanNo ratings yet
- Ruby Mae L. Aguaviva N32 1. Acute Pain: Assessment Diagnosis Planning Intervention Rationale EvaluationDocument9 pagesRuby Mae L. Aguaviva N32 1. Acute Pain: Assessment Diagnosis Planning Intervention Rationale EvaluationRuby Mae AguavivaNo ratings yet
- Pain ManagementDocument7 pagesPain ManagementHazel ZullaNo ratings yet
- Pain Lesson PlanDocument17 pagesPain Lesson PlanbharadwajjagreetiNo ratings yet
- NCP For Case Presentation (Acute Pain, Episiotomy)Document3 pagesNCP For Case Presentation (Acute Pain, Episiotomy)Jenny Ajoc100% (2)
- GAYO C. Revised NCPDocument7 pagesGAYO C. Revised NCPCarl LacambraNo ratings yet
- Nursing Care Plan: Clustered Cues Nursing Diagnosis Rationale Outcome Criteria Nursing Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Clustered Cues Nursing Diagnosis Rationale Outcome Criteria Nursing Interventions Rationale EvaluationCLEMENT, EUGENE CHADNo ratings yet
- Sample Nursing Care PlanDocument1 pageSample Nursing Care PlanQuiannë Delos ReyesNo ratings yet
- NCP Acute PainDocument2 pagesNCP Acute PainKhleanne CastilloNo ratings yet
- Acute PainDocument5 pagesAcute PainEricka MunsayacNo ratings yet
- This Chart Contains Information Provided by PatientsDocument4 pagesThis Chart Contains Information Provided by PatientsCecilia MendezNo ratings yet
- Pain Management Nursing Skills TypesDocument4 pagesPain Management Nursing Skills TypesBrittania CorbittNo ratings yet
- Managing Chronic Pain BiopsychosocialDocument169 pagesManaging Chronic Pain BiopsychosocialGabriel DelfinoNo ratings yet
- Ncm116 Lesson2 Rle Pain ManagementDocument4 pagesNcm116 Lesson2 Rle Pain ManagementMilcah NuylesNo ratings yet
- Pain assessment toolsDocument22 pagesPain assessment toolspuchioNo ratings yet
- Demonstrate: Pain Coping TechniquesDocument4 pagesDemonstrate: Pain Coping TechniquesMae Therese B. MAGNO100% (1)
- Nursing Care Plan Preoperative Cues Nursing Diagnosis Objectives Nursing Interventions Rationale Evaluation SubjectiveDocument5 pagesNursing Care Plan Preoperative Cues Nursing Diagnosis Objectives Nursing Interventions Rationale Evaluation SubjectiveShamsa AfdalNo ratings yet
- NCP For ChronicPain PDFDocument2 pagesNCP For ChronicPain PDFjay kusainNo ratings yet
- NCP Drug Study, Ojoy Dan Joshua LDocument2 pagesNCP Drug Study, Ojoy Dan Joshua Ldan.ojoy18No ratings yet
- Chap 10 - Lewis MSN Philippine 8eDocument26 pagesChap 10 - Lewis MSN Philippine 8eCHABELITA DAVIDNo ratings yet
- Nursing Care Plan - Acute Pain Assessment Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan - Acute Pain Assessment Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationNicole cuencosNo ratings yet
- Module 5 HA Pain Assessment The Fifth Vital SignsDocument12 pagesModule 5 HA Pain Assessment The Fifth Vital SignsCalvo AdrianNo ratings yet
- Midterms GeriaDocument18 pagesMidterms GeriaGiselle Estoquia100% (1)
- Nursing Care PlanDocument30 pagesNursing Care PlanJam CorrosNo ratings yet
- NCPDocument4 pagesNCPfairwoods90% (10)
- Question 1. Hypothetical Situation Which Includes Client's Assessment (History, Manifestations, Etc ) To Establish The ConditionDocument12 pagesQuestion 1. Hypothetical Situation Which Includes Client's Assessment (History, Manifestations, Etc ) To Establish The ConditionJoie JoieNo ratings yet
- PAIN FinalDocument23 pagesPAIN Finalneelimawanker chinnariNo ratings yet
- Nursing Intervention Reduces Abdominal PainDocument3 pagesNursing Intervention Reduces Abdominal PainNicole Mendonis LunarNo ratings yet
- NCPDocument6 pagesNCPAndrea Marie SevillaNo ratings yet
- The Somatic Toolkit: A Comprehensive Guide to Healing Trauma Through Somatic Practices: Unlock Your Body's Potential for Deep Healing and RestorationFrom EverandThe Somatic Toolkit: A Comprehensive Guide to Healing Trauma Through Somatic Practices: Unlock Your Body's Potential for Deep Healing and RestorationNo ratings yet
- Types of MalnutritionDocument8 pagesTypes of Malnutritionkazz!No ratings yet
- March 2016 (v2) QP - Paper 2 CIE Biology A-LevelDocument16 pagesMarch 2016 (v2) QP - Paper 2 CIE Biology A-LevelShazia AsifNo ratings yet
- Understanding Lewy Body DementiasDocument15 pagesUnderstanding Lewy Body DementiasCecilia Flores JaraNo ratings yet
- Acute Abdominal Pain History and Exam HPCDocument5 pagesAcute Abdominal Pain History and Exam HPCnaafNo ratings yet
- A Successful Case Study On Ayurvedic Management of HypothyroidismDocument6 pagesA Successful Case Study On Ayurvedic Management of HypothyroidismIJRASETPublicationsNo ratings yet
- Vitamin C and FatigueDocument7 pagesVitamin C and FatigueSteveNo ratings yet
- DR Vibhor PardasaniDocument19 pagesDR Vibhor PardasaniPushpanjali Crosslay HospitalNo ratings yet
- Discharge Plan Patient Teaching Pleural Effusion CastleDocument6 pagesDischarge Plan Patient Teaching Pleural Effusion Castleapi-341263362100% (2)
- MumpsDocument3 pagesMumpsAbeer FatimaNo ratings yet
- OsteoporoseDocument54 pagesOsteoporoseJandui DinizNo ratings yet
- CHD 128 Communicable Diseases and Control AssignmentDocument2 pagesCHD 128 Communicable Diseases and Control AssignmentDani AnyikaNo ratings yet
- Staphylococcus Aureus PhisiologyDocument21 pagesStaphylococcus Aureus PhisiologyJohann MuñozNo ratings yet
- Nama: Lubbul Aqil Maltuf (19010081) Dan Moh. Alvin Zalif F (19010091) Kelas: 19B Prodi: S1 Keperawatan Dialog: Asking Patient Medical HistoryDocument4 pagesNama: Lubbul Aqil Maltuf (19010081) Dan Moh. Alvin Zalif F (19010091) Kelas: 19B Prodi: S1 Keperawatan Dialog: Asking Patient Medical HistoryAll 17No ratings yet
- @slight - Cristobal v. Employees Compensation Commission, G.R. No. L-49280, Feb. 26, 1981Document9 pages@slight - Cristobal v. Employees Compensation Commission, G.R. No. L-49280, Feb. 26, 1981James OcampoNo ratings yet
- Social Determinants of HealthDocument2 pagesSocial Determinants of HealthKeerthi sanapala7278No ratings yet
- Perioralpigmentation PublishedDocument16 pagesPerioralpigmentation PublishedBrahmaiah UpputuriNo ratings yet
- Canine Viral Enteritis: Nipah and Hendra Virus InfectionsDocument9 pagesCanine Viral Enteritis: Nipah and Hendra Virus InfectionsAnnahi BcNo ratings yet
- Prepositions-Of-Time-Grammar-Guides - Sin RespuestaDocument1 pagePrepositions-Of-Time-Grammar-Guides - Sin RespuestaCarla BonanoNo ratings yet
- Assessment and Management of Patients With Endocrine DisordersDocument78 pagesAssessment and Management of Patients With Endocrine Disordershenny1620100% (1)
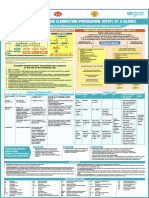
- NTEP at A Glance - Comprehensive Clinical Management Protocol For TBDocument1 pageNTEP at A Glance - Comprehensive Clinical Management Protocol For TBNael NajeebNo ratings yet
- Klebsiella Pneumoniae Pathogenesis: Etiology/BacteriologyDocument4 pagesKlebsiella Pneumoniae Pathogenesis: Etiology/Bacteriologysuper cute100% (1)
- NRSG 780 - Health Promotion and Population Health: Module 3: EpidemiologyDocument34 pagesNRSG 780 - Health Promotion and Population Health: Module 3: EpidemiologyjustdoyourNo ratings yet
- Davainea Proglottina - A Potentially Underestimated PDFDocument3 pagesDavainea Proglottina - A Potentially Underestimated PDFryan100% (1)
- Schizophrenia Clinical Presentation - History, Physical Examination, ComplicationsDocument4 pagesSchizophrenia Clinical Presentation - History, Physical Examination, ComplicationsdilaNo ratings yet
- Clinical Review: The Management of Lower Urinary Tract Symptoms in MenDocument4 pagesClinical Review: The Management of Lower Urinary Tract Symptoms in MenSan Phạm ĐìnhNo ratings yet
- CARDIOVASCULAR EXAMINATION Human DiseaseDocument4 pagesCARDIOVASCULAR EXAMINATION Human DiseaseVictoria MedfordNo ratings yet