You might also like
- Conquering Pain: How to Prevent It, Treat It and Lead a Better LifeFrom EverandConquering Pain: How to Prevent It, Treat It and Lead a Better LifeRating: 5 out of 5 stars5/5 (1)
- The Art of Holistic Pain Management: A Practical HandbookFrom EverandThe Art of Holistic Pain Management: A Practical HandbookNo ratings yet
- Nursing Care Plan for Acute PainDocument2 pagesNursing Care Plan for Acute Painunnamed person100% (1)
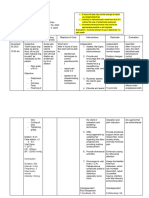
- Nursing Care Plan - Acute Pain Assessment Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan - Acute Pain Assessment Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationNicole cuencosNo ratings yet
- Typhoid Fever NCPDocument46 pagesTyphoid Fever NCPLyra Lustre RN67% (3)
- Post-CS Nursing Care Plan GoalsDocument7 pagesPost-CS Nursing Care Plan GoalsshinloNo ratings yet
- Nursing Care Plan for Labor Pain ManagementDocument3 pagesNursing Care Plan for Labor Pain ManagementFc CrisostomoNo ratings yet
- Kusain - NCP in NCM 112 RleDocument2 pagesKusain - NCP in NCM 112 Rlejay kusainNo ratings yet
- Case Scenario 5 NCPDocument10 pagesCase Scenario 5 NCPkdfhjfhfNo ratings yet
- NCP Acute PainDocument2 pagesNCP Acute PainMillicent Faye G. Gelit50% (2)
- NCPDocument4 pagesNCPJhuRise Ann ManganaNo ratings yet
- UntitledDocument5 pagesUntitledJayelles Dixien JuguilonNo ratings yet
- Source: Operating Room Technique by Nancymarie PhillipsDocument1 pageSource: Operating Room Technique by Nancymarie Phillipsnoreen ellieNo ratings yet
- Case Study No.10 (NCP)Document5 pagesCase Study No.10 (NCP)Rosemarie R. Reyes100% (1)
- Assessments Nursing Diagnosis Planning Interventions Rationale EvaluationDocument12 pagesAssessments Nursing Diagnosis Planning Interventions Rationale EvaluationAsniah Hadjiadatu AbdullahNo ratings yet
- NCP Post OpDocument4 pagesNCP Post OpNIKKI CARYL ZAFRANo ratings yet
- Assessment Nursing Diagnosis Scientific Explanation Planning Intervention Rationale Evaluation IndeoendentDocument3 pagesAssessment Nursing Diagnosis Scientific Explanation Planning Intervention Rationale Evaluation IndeoendentDiane Sarino CabonceNo ratings yet
- Nursing interventions for pain and nutrition managementDocument8 pagesNursing interventions for pain and nutrition managementNyeam NyeamNo ratings yet
- NCP-PAIN-1Document6 pagesNCP-PAIN-1goodemonz15No ratings yet
- NCP Charm EditedDocument6 pagesNCP Charm EditedampogeNo ratings yet
- Emmy's NCP and EtcDocument7 pagesEmmy's NCP and EtcabraNo ratings yet
- Nursing Care Plan For CholecystitisDocument4 pagesNursing Care Plan For CholecystitisEemyaj Jaymee88% (8)
- NCP Acute PainDocument3 pagesNCP Acute PainBasema HashhashNo ratings yet
- Ruby Mae L. Aguaviva N32 1. Acute Pain: Assessment Diagnosis Planning Intervention Rationale EvaluationDocument9 pagesRuby Mae L. Aguaviva N32 1. Acute Pain: Assessment Diagnosis Planning Intervention Rationale EvaluationRuby Mae AguavivaNo ratings yet
- Nursing Assessment and Interventions for Acute Chest PainDocument3 pagesNursing Assessment and Interventions for Acute Chest PainAjay SupanNo ratings yet
- Nursing Care Plan AppendicitisDocument2 pagesNursing Care Plan Appendicitisderic95% (57)
- Nursing Care Plan for Post-Surgical Pain ManagementDocument7 pagesNursing Care Plan for Post-Surgical Pain ManagementMacris BondocNo ratings yet
- College Nursing Care Plan TemplateDocument9 pagesCollege Nursing Care Plan TemplateCecil MonteroNo ratings yet
- Nursing Care Plan: Clustered Cues Nursing Diagnosis Rationale Outcome Criteria Nursing Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Clustered Cues Nursing Diagnosis Rationale Outcome Criteria Nursing Interventions Rationale EvaluationCLEMENT, EUGENE CHADNo ratings yet
- Final Zollinger-Ellison SyndromeDocument9 pagesFinal Zollinger-Ellison SyndromeGLYDEL CORDERONo ratings yet
- Nursing Care Plan2Document3 pagesNursing Care Plan2gaeLtorvzNo ratings yet
- Heart Clinic: Alternative Learning System Related Learning ExperienceDocument8 pagesHeart Clinic: Alternative Learning System Related Learning ExperienceEdson John DemayoNo ratings yet
- Nutrition Management for Zollinger-Ellison PatientDocument9 pagesNutrition Management for Zollinger-Ellison PatientGLYDEL CORDERONo ratings yet
- Assessment Nursing Diagnosis Planning Nursing Intervntion Rationale EvaluationDocument3 pagesAssessment Nursing Diagnosis Planning Nursing Intervntion Rationale EvaluationDeinielle Magdangal RomeroNo ratings yet
- Flank Pain, Anxiety...Document7 pagesFlank Pain, Anxiety...reneighdNo ratings yet
- Care PlanDocument2 pagesCare PlanAnonymous 9QBCcNNo ratings yet
- Osteoporosis Prognosis and Nursing CareDocument4 pagesOsteoporosis Prognosis and Nursing CareJanine Mae MacaraigNo ratings yet
- Gouty NCPDocument9 pagesGouty NCPKrishelle Kate PannigNo ratings yet
- Nursing Diagnosis, Goals, and Interventions for Acute Pain, Nutrition Imbalance, and Fluid Volume DeficitDocument5 pagesNursing Diagnosis, Goals, and Interventions for Acute Pain, Nutrition Imbalance, and Fluid Volume DeficitAngelica ValeraNo ratings yet
- Nursing Care PlanDocument5 pagesNursing Care PlankingpinNo ratings yet
- Cues Nursing Diagnosis Goals and Objectives Nursing Interventions Rationale Evaluation IndependentDocument1 pageCues Nursing Diagnosis Goals and Objectives Nursing Interventions Rationale Evaluation IndependentSitti ZhainabNo ratings yet
- NCP Activity NavidasDocument2 pagesNCP Activity NavidasFran LanNo ratings yet
- College of Health Sciences Nursing Care Plan for Acute Myocardial InfarctionDocument4 pagesCollege of Health Sciences Nursing Care Plan for Acute Myocardial InfarctionLouise GudmalinNo ratings yet
- Forro Intestinal ObstructionDocument3 pagesForro Intestinal ObstructionShiehan Mae ForroNo ratings yet
- Assessment Diagnosis Scientific Basis Planning Nursing Interventions Rationale EvaluationDocument3 pagesAssessment Diagnosis Scientific Basis Planning Nursing Interventions Rationale EvaluationGj PaguidianNo ratings yet
- Group 9 Sickle Cell Anemia Case Study ActivityDocument4 pagesGroup 9 Sickle Cell Anemia Case Study ActivityJuliaNo ratings yet
- NCP CholelithiasisDocument6 pagesNCP CholelithiasisWendy Hingpit RonquilloNo ratings yet
- Name: Babu Kaji Maharjan: Patient's IdentificationDocument6 pagesName: Babu Kaji Maharjan: Patient's IdentificationAlisha MaharjanNo ratings yet
- Nursing Theorists of Historical Significance - NotesDocument36 pagesNursing Theorists of Historical Significance - NotesSARABIA, ARVIN JR.No ratings yet
- CaseDocument3 pagesCasebLessy_july16No ratings yet
- Subjective: Sto: Diagnostic:: Assessme NT Explanatio Nofthe Problem Planning Interven Tion Rationale Evaluati ONDocument3 pagesSubjective: Sto: Diagnostic:: Assessme NT Explanatio Nofthe Problem Planning Interven Tion Rationale Evaluati ONRona PieNo ratings yet
- Secrets of Healer - Magic of Reflexology: Magic of ReflexologyFrom EverandSecrets of Healer - Magic of Reflexology: Magic of ReflexologyNo ratings yet
- Pain Relief without Drugs: A Self-Help Guide for Chronic Pain and TraumaFrom EverandPain Relief without Drugs: A Self-Help Guide for Chronic Pain and TraumaNo ratings yet
- Trigger Point Therapy for Myofascial Pain: The Practice of Informed TouchFrom EverandTrigger Point Therapy for Myofascial Pain: The Practice of Informed TouchRating: 4 out of 5 stars4/5 (5)
- Holistic Pain Relief: How to ease muscles, joints and other painful conditionsFrom EverandHolistic Pain Relief: How to ease muscles, joints and other painful conditionsNo ratings yet
- The Journey to Pain Relief: A Hands-On Guide to Breakthroughs in Pain TreatmentFrom EverandThe Journey to Pain Relief: A Hands-On Guide to Breakthroughs in Pain TreatmentRating: 4.5 out of 5 stars4.5/5 (3)
- Natural Pain Relief: How to Soothe and Dissolve Physical Pain with MindfulnessFrom EverandNatural Pain Relief: How to Soothe and Dissolve Physical Pain with MindfulnessRating: 4 out of 5 stars4/5 (5)
- Theories of Development Mental and Developmental FunctionDocument9 pagesTheories of Development Mental and Developmental FunctionAndrea Marie SevillaNo ratings yet
- Sevilla, A. - Nursing Informatics AssignmentDocument4 pagesSevilla, A. - Nursing Informatics AssignmentAndrea Marie SevillaNo ratings yet
- Nurses Progress Notes for Kaoru T. PasyenteDocument3 pagesNurses Progress Notes for Kaoru T. PasyenteAndrea Marie Sevilla100% (1)
- Sevilla, A. - Nursing Informatics AssignmentDocument4 pagesSevilla, A. - Nursing Informatics AssignmentAndrea Marie SevillaNo ratings yet
- The Childbearing Childbearing Family in The Community MCNDocument9 pagesThe Childbearing Childbearing Family in The Community MCNAndrea Marie SevillaNo ratings yet
- Fetal Assessment 1Document7 pagesFetal Assessment 1Andrea Marie SevillaNo ratings yet
- First Lecture - Nursing InfoDocument3 pagesFirst Lecture - Nursing InfoAndrea Marie SevillaNo ratings yet
- The Family and Family Health: Prepared By: Vivian A. Cezar, RN 9/24/2020 NCM 107: Maternal & Child HealthDocument62 pagesThe Family and Family Health: Prepared By: Vivian A. Cezar, RN 9/24/2020 NCM 107: Maternal & Child HealthAndrea Marie SevillaNo ratings yet
- A Practical Approach To Preventing Child Deaths: What The Pediatrician Can DoDocument44 pagesA Practical Approach To Preventing Child Deaths: What The Pediatrician Can DoSophia Loraine Dorone JesuraNo ratings yet
- Theories of Development Mental and Developmental FunctionDocument9 pagesTheories of Development Mental and Developmental FunctionAndrea Marie SevillaNo ratings yet
- Labor and DeliveryDocument6 pagesLabor and DeliveryAndrea Marie SevillaNo ratings yet
- Implementing Family Care PlanDocument6 pagesImplementing Family Care PlanAndrea Marie SevillaNo ratings yet
- Potassium Chloride Mechanism, Indications, Side EffectsDocument4 pagesPotassium Chloride Mechanism, Indications, Side EffectsAndrea Marie SevillaNo ratings yet
- NCP - SevillaDocument7 pagesNCP - SevillaAndrea Marie SevillaNo ratings yet
- Drug StudyDocument5 pagesDrug StudyAndrea Marie SevillaNo ratings yet
- NCP 1Document3 pagesNCP 1Andrea Marie SevillaNo ratings yet
- Impaired Oral Mucous Membrane Integrity Related To DehydrationDocument1 pageImpaired Oral Mucous Membrane Integrity Related To DehydrationAndrea Marie SevillaNo ratings yet
- Reproductive Life Planning - YcremDocument7 pagesReproductive Life Planning - YcremAndrea Marie SevillaNo ratings yet
- Theories of Development Mental and Developmental FunctionDocument9 pagesTheories of Development Mental and Developmental FunctionAndrea Marie SevillaNo ratings yet
- Reproductive Life Planning - YcremDocument7 pagesReproductive Life Planning - YcremAndrea Marie SevillaNo ratings yet
- The Family and Family Health: Prepared By: Vivian A. Cezar, RN 9/24/2020 NCM 107: Maternal & Child HealthDocument62 pagesThe Family and Family Health: Prepared By: Vivian A. Cezar, RN 9/24/2020 NCM 107: Maternal & Child HealthAndrea Marie SevillaNo ratings yet
- The Childbearing Childbearing Family in The Community MCNDocument9 pagesThe Childbearing Childbearing Family in The Community MCNAndrea Marie SevillaNo ratings yet
- MCN Family Health Maam VivDocument5 pagesMCN Family Health Maam VivAndrea Marie SevillaNo ratings yet
- Providing Comfort During LaborDocument11 pagesProviding Comfort During LaborAndrea Marie SevillaNo ratings yet
- Providing Comfort During LaborDocument11 pagesProviding Comfort During LaborAndrea Marie SevillaNo ratings yet
- MCN - The Childbearing and Childbearing Family in The CommunityDocument91 pagesMCN - The Childbearing and Childbearing Family in The CommunityAndrea Marie SevillaNo ratings yet
- Labor and DeliveryDocument6 pagesLabor and DeliveryAndrea Marie SevillaNo ratings yet
- Labor and DeliveryDocument7 pagesLabor and DeliveryAndrea Marie SevillaNo ratings yet
- Fetal Assessment 1Document7 pagesFetal Assessment 1Andrea Marie SevillaNo ratings yet
- BOF, LF & CasterDocument14 pagesBOF, LF & CastermaklesurrahmanNo ratings yet
- Grade 3 science syllabus 1st and 2nd semesterDocument2 pagesGrade 3 science syllabus 1st and 2nd semesterelyzabeth SibaraniNo ratings yet
- Iso 28000Document11 pagesIso 28000Aida FatmawatiNo ratings yet
- 9 To 5 Props PresetsDocument4 pages9 To 5 Props Presetsapi-300450266100% (1)
- SCE Research Paper PDFDocument12 pagesSCE Research Paper PDFmuoi2002No ratings yet
- AAR Maintenance 001Document3 pagesAAR Maintenance 001prakash reddyNo ratings yet
- LAST CARGOES AND CLEANINGDocument1 pageLAST CARGOES AND CLEANINGAung Htet KyawNo ratings yet
- Switzerland: Food and CultureDocument18 pagesSwitzerland: Food and CultureAaron CoutinhoNo ratings yet
- Grab Go Porter S 5 ForcesDocument2 pagesGrab Go Porter S 5 ForcesUtkarsh SharmaNo ratings yet
- VIDEO 2 - Thì hiện tại tiếp diễn và hiện tại hoàn thànhDocument3 pagesVIDEO 2 - Thì hiện tại tiếp diễn và hiện tại hoàn thànhÝ Nguyễn NhưNo ratings yet
- Pet - WikipediaDocument12 pagesPet - Wikipediabdalcin5512No ratings yet
- UNICESS KR Consmetics Maeteria Nunssupjara 01apr23Document44 pagesUNICESS KR Consmetics Maeteria Nunssupjara 01apr23ZB ChuaNo ratings yet
- Copia de Tissue Response To Dental CariesDocument7 pagesCopia de Tissue Response To Dental Cariesjorefe12No ratings yet
- Benefits at Cognizant Technology SolutionsDocument5 pagesBenefits at Cognizant Technology Solutions8130089011No ratings yet
- Stress and FilipinosDocument28 pagesStress and FilipinosDaniel John Arboleda100% (2)
- Fundamentals of Fast SwimmingDocument9 pagesFundamentals of Fast SwimmingTorcay Ulucay100% (1)
- Completed Manuscript 1 5Document52 pagesCompleted Manuscript 1 5SAMANTHA LACABANo ratings yet
- Design and Built-A4Document2 pagesDesign and Built-A4farahazuraNo ratings yet
- GTT Module 5Document156 pagesGTT Module 5ABDULRAHIMAN RAJEKHANNo ratings yet
- The Ultimate Safari (A Short Story)Document20 pagesThe Ultimate Safari (A Short Story)David AlcasidNo ratings yet
- Model Fs CatalogDocument4 pagesModel Fs CatalogThomas StempienNo ratings yet
- of Types of Nuclear ReactorDocument33 pagesof Types of Nuclear Reactormandhir67% (3)
- 8-26-16 Police ReportDocument14 pages8-26-16 Police ReportNoah StubbsNo ratings yet
- Test Report OD63mm PN12.5 PE100Document6 pagesTest Report OD63mm PN12.5 PE100Im ChinithNo ratings yet
- WSO 2022 IB Working Conditions SurveyDocument42 pagesWSO 2022 IB Working Conditions SurveyPhạm Hồng HuếNo ratings yet
- EO On Ban of Fireworks (Integrated)Document2 pagesEO On Ban of Fireworks (Integrated)Mario Roldan Jr.No ratings yet
- Cellular Basis of HeredityDocument12 pagesCellular Basis of HeredityLadyvirdi CarbonellNo ratings yet
- Infinite & Finite Slope1Document38 pagesInfinite & Finite Slope1CHUKKALA LEELA RAVALINo ratings yet
- HR Policy For Hotel IndustriesDocument5 pagesHR Policy For Hotel IndustriesHR Forum India78% (9)
- Circulatory System Packet BDocument5 pagesCirculatory System Packet BLouise SalvadorNo ratings yet