You might also like
- Hazardous Explosives Areasv0Document34 pagesHazardous Explosives Areasv0macodarvNo ratings yet
- Powershift Transmissions PDFDocument39 pagesPowershift Transmissions PDFfernando chinchazo100% (1)
- Magazine Fit ChartDocument4 pagesMagazine Fit Chartcloudman81No ratings yet
- Starting An Intravenous InfusionDocument2 pagesStarting An Intravenous InfusionAmiel Francisco Reyes100% (1)
- Scrubbing, Gowning and GlovingDocument4 pagesScrubbing, Gowning and Glovingjgcriste85% (20)
- Attire, Surgical Scrub, Gowning and GlovingDocument23 pagesAttire, Surgical Scrub, Gowning and GlovingRumelle ReyesNo ratings yet
- College of Nursing - Clinical Nursing Skills ChecklistDocument128 pagesCollege of Nursing - Clinical Nursing Skills ChecklistAya Abulag100% (2)
- Persons and Family Relations Reviewer SluDocument98 pagesPersons and Family Relations Reviewer SluKing Monteclaro Montereal100% (1)
- Employee Engagement and Motivation A Case StudyDocument20 pagesEmployee Engagement and Motivation A Case StudyA. Karlina Askarini MakkasauNo ratings yet
- Surgical Scrub Gown and Glove Procedures Policy 201310Document17 pagesSurgical Scrub Gown and Glove Procedures Policy 201310Anonymous mvNUtwidNo ratings yet
- Operating NURSEDocument8 pagesOperating NURSEAlexis de los SantosNo ratings yet
- Surgical Handwashing Resource Material 2023-2024Document9 pagesSurgical Handwashing Resource Material 2023-2024Cherry Louise O. SanvictoresNo ratings yet
- Assisted Gowning & GlovingDocument12 pagesAssisted Gowning & GlovingCarmina GurreaNo ratings yet
- Aseptic TechniqueDocument15 pagesAseptic Techniquerhizalyn13No ratings yet
- 12 Steps of Aseptic TechniqueDocument7 pages12 Steps of Aseptic TechniqueRobbie MejiaNo ratings yet
- Gowning and GlovingDocument2 pagesGowning and GlovingVictoria Castillo TamayoNo ratings yet
- Gowning and Gloving Surgical HandwshingDocument9 pagesGowning and Gloving Surgical HandwshingHazzel Mae ZaportizaNo ratings yet
- Scrubbing Gowning and Gloving LECTUREDocument5 pagesScrubbing Gowning and Gloving LECTUREEyji GeronimoNo ratings yet
- 13 Aseptic TechniqueDocument6 pages13 Aseptic TechniqueaironmaeNo ratings yet
- Surgical Gowning and GlovingDocument15 pagesSurgical Gowning and GlovingAllyssa MackinnonNo ratings yet
- Surgical Skin Prep PDFDocument12 pagesSurgical Skin Prep PDFDrrjdrjd MemeNo ratings yet
- Skin Preparation FinalDocument4 pagesSkin Preparation FinalJerson EdilloNo ratings yet
- Preparing A Sterile FieldDocument11 pagesPreparing A Sterile FieldjeremiahNo ratings yet
- Principles of Sterile TechniqueDocument2 pagesPrinciples of Sterile TechniqueAliah M. AngodNo ratings yet
- Principles of Sterile TechniqueDocument3 pagesPrinciples of Sterile Techniquegaylenice100% (2)
- Pre-Operative Nursing CareDocument79 pagesPre-Operative Nursing CarePeter FrimpongNo ratings yet
- Basic Principles of Surgical AsepsisDocument1 pageBasic Principles of Surgical AsepsisAsiah IsmailNo ratings yet
- Principles of Surgical AsepsisDocument54 pagesPrinciples of Surgical Asepsisbibeksd796100% (6)
- What Is Aseptic TechniqueDocument11 pagesWhat Is Aseptic TechniqueMarlchiel Nathan ArregladoNo ratings yet
- Operating Room InstrumentsDocument8 pagesOperating Room InstrumentsVictoria Castillo TamayoNo ratings yet
- GENERAL SAFETY CHECKLIST GuidelinesDocument10 pagesGENERAL SAFETY CHECKLIST GuidelinesTina AlteranNo ratings yet
- Surgical Scrub, Gowning and Glovingsurgical ScrubDocument5 pagesSurgical Scrub, Gowning and Glovingsurgical ScrubMuhammad TohaNo ratings yet
- Duties or NurseDocument10 pagesDuties or NursehailleyannNo ratings yet
- Surgical Scrubbing Checklist - EVANGELISTADocument6 pagesSurgical Scrubbing Checklist - EVANGELISTAGabrielle EvangelistaNo ratings yet
- 5 Principles of Aseptic Technique PDFDocument23 pages5 Principles of Aseptic Technique PDFAron NovesterosNo ratings yet
- Gowning GlovingDocument37 pagesGowning GlovingMark Arryson CasisonNo ratings yet
- Wound Care and Dressing ChecklistDocument4 pagesWound Care and Dressing ChecklistGelo BallartaNo ratings yet
- Wound CareDocument3 pagesWound Caregrangerhermionep100% (1)
- OR Duty RLE RequirementsDocument5 pagesOR Duty RLE RequirementsSammy Jr FamilarNo ratings yet
- Complete Bed Bath2Document3 pagesComplete Bed Bath2rufino delacruzNo ratings yet
- Calamba Doctors' College: Bachelor of Science in NursingDocument3 pagesCalamba Doctors' College: Bachelor of Science in NursingDaniel Daniel100% (1)
- Assess Patient Data Such As Vital Signs, Laboratory Values, and Allergies Before Preparing and Administering Medications by InjectionDocument12 pagesAssess Patient Data Such As Vital Signs, Laboratory Values, and Allergies Before Preparing and Administering Medications by InjectionLRBNo ratings yet
- Procedures and RationaleDocument7 pagesProcedures and RationaleMonmon BagarinaoNo ratings yet
- CATHETERIZATIONDocument13 pagesCATHETERIZATIONSarah Uy Caronan100% (1)
- Perioperative Nursing Skills and Procedure PDFDocument4 pagesPerioperative Nursing Skills and Procedure PDFRouwi DesiatcoNo ratings yet
- Gloving by Open Glove TechniqueDocument5 pagesGloving by Open Glove TechniqueRoselle Farolan LopezNo ratings yet
- IntraOperative Nursing ManagementDocument7 pagesIntraOperative Nursing ManagementAl-nazer Azer Al100% (2)
- Etiquette and PrinciplesDocument3 pagesEtiquette and PrinciplesHoney Bee S. PlatolonNo ratings yet
- What Are The Functions of A Scrub NurseDocument24 pagesWhat Are The Functions of A Scrub NurseBrigette Jane Michelle Martil100% (1)
- Intraoperative 2Document104 pagesIntraoperative 2Mark Arryson CasisonNo ratings yet
- Tracheostomy CareDocument1 pageTracheostomy CareShreyas WalvekarNo ratings yet
- Sputum CollectionDocument5 pagesSputum CollectionChejsalm AlvarezNo ratings yet
- Sultan Kudarat State University College of Health SciencesDocument7 pagesSultan Kudarat State University College of Health SciencesRheal P EsmailNo ratings yet
- Perioperative Nursing: Bryan Joven C. Ong, RN, MSNDocument35 pagesPerioperative Nursing: Bryan Joven C. Ong, RN, MSNAngelica RicoNo ratings yet
- Wound Care ChecklistDocument5 pagesWound Care Checklistacademic purposes100% (1)
- Parenteral Administration ChecklistDocument37 pagesParenteral Administration ChecklistFregen Mae ApoyaNo ratings yet
- Perform Hand Hygiene: Don Goggle or Face ShieldDocument2 pagesPerform Hand Hygiene: Don Goggle or Face ShieldKnox Axton Kaden100% (1)
- CatheterizationDocument3 pagesCatheterizationLizzy WayNo ratings yet
- Dilation and CurettageDocument4 pagesDilation and CurettageFernandez, Florence NicoleNo ratings yet
- Surgical Aseptic Technique Sterile FieldDocument18 pagesSurgical Aseptic Technique Sterile FieldAsiah IsmailNo ratings yet
- Oral Care ProtocolDocument8 pagesOral Care ProtocolQonitaNurMiladiNo ratings yet
- Or Rle 1-1Document23 pagesOr Rle 1-1Jan Federick Bantay100% (1)
- Bed Bath Procedure ChecklistDocument4 pagesBed Bath Procedure ChecklistMarku LeeNo ratings yet
- Aseptic TechniqueDocument9 pagesAseptic TechniqueFaith IriemiNo ratings yet
- Operating RoomDocument4 pagesOperating RoomKristine Anne Liquiran Avenado100% (1)
- Compost PitDocument3 pagesCompost PitIan Rose EnomarNo ratings yet
- Ai Unit 5Document138 pagesAi Unit 5Ronit SinghNo ratings yet
- The United States Supreme Court - 1948-1949Document56 pagesThe United States Supreme Court - 1948-1949Tomás AguerreNo ratings yet
- HKIHT Road and Infra 5 FlyerDocument3 pagesHKIHT Road and Infra 5 FlyerWai TszYanNo ratings yet
- API Standard 653 - Tank Inspection, Repair, Alteration, and ReconstructionDocument15 pagesAPI Standard 653 - Tank Inspection, Repair, Alteration, and ReconstructionMuhammad Nasir SiddiqueNo ratings yet
- Taylor Ice Cream Machine150Document77 pagesTaylor Ice Cream Machine150blascool8No ratings yet
- OSDIDocument34 pagesOSDIImam Nur ShodiqNo ratings yet
- NM QuadraticDocument4 pagesNM Quadraticvenice wxNo ratings yet
- 3 Mitsubishi-OUTLANDER-2006-BODY-REPAIR-MANUAL-WELDED-PANEL-REPLACEMENTDocument36 pages3 Mitsubishi-OUTLANDER-2006-BODY-REPAIR-MANUAL-WELDED-PANEL-REPLACEMENTClodoaldo BiassioNo ratings yet
- pFMS2 PDFDocument64 pagespFMS2 PDFFaizanTariqFTNo ratings yet
- Gantry SystemDocument4 pagesGantry SystemTh NattapongNo ratings yet
- SKN 240, SKR 240: Rectifier DiodeDocument3 pagesSKN 240, SKR 240: Rectifier DiodeSidnei de Souza MartinsNo ratings yet
- Wargames Illustrated #019Document60 pagesWargames Illustrated #019Анатолий Золотухин50% (2)
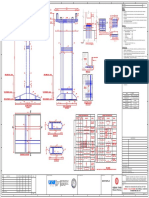
- Typical Plan For Pedestal: Mbpl-Pgipl JVDocument1 pageTypical Plan For Pedestal: Mbpl-Pgipl JVSaurabh PandeyNo ratings yet
- RINA Performance of Protective Coating in Ballast Tanks - Where A Class Society Can HelpDocument49 pagesRINA Performance of Protective Coating in Ballast Tanks - Where A Class Society Can HelpJorge Alberto Montalat100% (1)
- Cost BehaviorDocument11 pagesCost BehaviorfelipemagalhaeslemosNo ratings yet
- Account Test IncrementDocument2 pagesAccount Test IncrementVenkatesanSelvarajNo ratings yet
- Forms of Arbitration AgreementDocument8 pagesForms of Arbitration AgreementPreeminentPriyankaNo ratings yet
- Civil Engineering Hydraulics 5th EditionDocument7 pagesCivil Engineering Hydraulics 5th EditionChris ChrisNo ratings yet
- ការងាររៀបចំក្រុមហ៊ុនDocument4 pagesការងាររៀបចំក្រុមហ៊ុនPottynanarak SovannNo ratings yet
- ER200-A5EC16997 Rev 0Document1 pageER200-A5EC16997 Rev 0MarionNo ratings yet
- Nfpa Compliance Inspection Checklist A361Document8 pagesNfpa Compliance Inspection Checklist A361gerardtrNo ratings yet
- hp-300 Series BrochureDocument5 pageshp-300 Series BrochureGianfranco DyNo ratings yet
- 10 Acknowledgement SlipDocument1 page10 Acknowledgement SlipumarsaboNo ratings yet
- Report - Solicitation LetterDocument5 pagesReport - Solicitation LetterShinjiNo ratings yet