You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Periodontal FlapDocument43 pagesThe Periodontal FlapDeb SNo ratings yet
- NEBDN Dental Charting Book APRIL 2015Document13 pagesNEBDN Dental Charting Book APRIL 2015Avita RathNo ratings yet
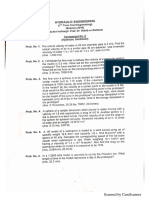
- Hydraulic Lab Manual 2017Document48 pagesHydraulic Lab Manual 2017Muhammad AdilNo ratings yet
- Linear OcclusionDocument8 pagesLinear OcclusionAmar BhochhibhoyaNo ratings yet
- Clinical Success in Resin Bonded Bridges PDFDocument7 pagesClinical Success in Resin Bonded Bridges PDFNajeeb UllahNo ratings yet
- Buku Panduan UkgmDocument53 pagesBuku Panduan UkgmNurul HidayahNo ratings yet
- Anterior Wax UpDocument3 pagesAnterior Wax Upalioossa100% (2)
- First Approximate Method of Design For Compression Failure Step 3Document51 pagesFirst Approximate Method of Design For Compression Failure Step 3Muhammad AdilNo ratings yet
- Feasibility Analysis: Bruce R. Barringer R. Duane IrelandDocument43 pagesFeasibility Analysis: Bruce R. Barringer R. Duane IrelandMuhammad AdilNo ratings yet
- PRC-II Columns LEC-1Document53 pagesPRC-II Columns LEC-1Muhammad AdilNo ratings yet
- Complex Engineering Problem Fall 2019 HE, CE-432Document1 pageComplex Engineering Problem Fall 2019 HE, CE-432Muhammad AdilNo ratings yet
- Hydraulics (Assignment 6)Document2 pagesHydraulics (Assignment 6)Muhammad AdilNo ratings yet
- Complex Engineering Problem Fall 2019 HE, CE-432Document1 pageComplex Engineering Problem Fall 2019 HE, CE-432Muhammad Adil100% (1)
- Admission Form CCKK 2020 2Document1 pageAdmission Form CCKK 2020 2Ubaid TariqNo ratings yet
- PUBGMOBILE OfficialCampus Championship 2021 PKDocument41 pagesPUBGMOBILE OfficialCampus Championship 2021 PKMuhammad AdilNo ratings yet
- Universal Life and Gaming Earbuds: The Finest Sound Experience MEMS Mic With Universal Control ButtonDocument2 pagesUniversal Life and Gaming Earbuds: The Finest Sound Experience MEMS Mic With Universal Control ButtonMuhammad AdilNo ratings yet
- 5.0 Poisson - S Ratio and Theories of Failure (Updated)Document21 pages5.0 Poisson - S Ratio and Theories of Failure (Updated)Muhammad AdilNo ratings yet
- Strengthening Sand Column Using PFA-Cement Mixture: Mustafa YDocument10 pagesStrengthening Sand Column Using PFA-Cement Mixture: Mustafa YMuhammad AdilNo ratings yet
- 4.0 Strain TrasnformationDocument28 pages4.0 Strain TrasnformationMuhammad AdilNo ratings yet
- 4.1 Mohr - S Circle For Strain RosetteDocument6 pages4.1 Mohr - S Circle For Strain RosetteMuhammad AdilNo ratings yet
- Earthquake: Earthquake Hazard/Disaster ManagementDocument5 pagesEarthquake: Earthquake Hazard/Disaster ManagementMuhammad AdilNo ratings yet
- 3.0 Mohr - S Circle (Plane Stress)Document10 pages3.0 Mohr - S Circle (Plane Stress)Muhammad AdilNo ratings yet
- Disaster Loss Database-1Document3 pagesDisaster Loss Database-1Muhammad AdilNo ratings yet
- Development of Occlusion: Gum Pads StageDocument5 pagesDevelopment of Occlusion: Gum Pads StageSaid SaidNo ratings yet
- Sealing Ability of Zinc Oxide Eugenol and Non-Eugenol-Based Temporary FillingDocument6 pagesSealing Ability of Zinc Oxide Eugenol and Non-Eugenol-Based Temporary FillingTahir TahirNo ratings yet
- Comfort Dental Fee-Schedule-MO-KS-2014-accessibleDocument1 pageComfort Dental Fee-Schedule-MO-KS-2014-accessibleAllen WilburNo ratings yet
- Swing Lock Partial DentureDocument22 pagesSwing Lock Partial DentureSanNo ratings yet
- Brazilian Board of Orthodontics and Facial Orthopedics: Certifying ExcellenceDocument10 pagesBrazilian Board of Orthodontics and Facial Orthopedics: Certifying ExcellenceHanindyaNoorAgusthaNo ratings yet
- Oral Anatomy Lecture 2 Tooth and Its Supporting StructureDocument73 pagesOral Anatomy Lecture 2 Tooth and Its Supporting StructurePhoelise SalazarNo ratings yet
- Arco Facial ARTICLUO INGELSDocument10 pagesArco Facial ARTICLUO INGELSruthy arias anahuaNo ratings yet
- Variolink NDocument18 pagesVariolink NThaer Saad Al DeenNo ratings yet
- CBCT Patterns of Bone Loss and Clinical Predictors For The Diagnosis of Cracked Teeth and Teeth With Vertical Root FractureDocument7 pagesCBCT Patterns of Bone Loss and Clinical Predictors For The Diagnosis of Cracked Teeth and Teeth With Vertical Root FractureAssem HNo ratings yet
- Oral Hygiene Toothbrush One Cycle Per SecondDocument3 pagesOral Hygiene Toothbrush One Cycle Per SecondjunquelalaNo ratings yet
- Dental ElevatorsDocument28 pagesDental ElevatorsTejaswiniNo ratings yet
- Biotype and BioformDocument6 pagesBiotype and Bioformilich sevillaNo ratings yet
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDocument39 pagesAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyNo ratings yet
- Saade 2015Document21 pagesSaade 2015divyaNo ratings yet
- Quadri HeliceDocument12 pagesQuadri HeliceMartin AdriazolaNo ratings yet
- Interproximal Enamel Reduction in Comprehensive Orthodontic Treatment: A ReviewDocument4 pagesInterproximal Enamel Reduction in Comprehensive Orthodontic Treatment: A ReviewBasuni RahmanNo ratings yet
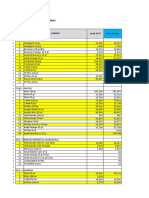
- Bahan Kemas - Selisih SO Vs Sistem FY2020 - 291220Document17 pagesBahan Kemas - Selisih SO Vs Sistem FY2020 - 291220Idan RidwanNo ratings yet
- ADK GuideDocument21 pagesADK GuideZayd DeenNo ratings yet
- Evolution of Mandibulomaxillary FixationDocument32 pagesEvolution of Mandibulomaxillary FixationFahad QiamNo ratings yet
- The Current State of Chairside Digital Dentistry and MaterialsDocument23 pagesThe Current State of Chairside Digital Dentistry and MaterialsJorge AlvaradoNo ratings yet
- Rinchuse 2006Document8 pagesRinchuse 2006jhon HanselNo ratings yet
- Significance of Facebow TransferDocument5 pagesSignificance of Facebow Transfermedicalrecords211No ratings yet
- Dental Implant Prosthetics Carl e Misch .12Document3 pagesDental Implant Prosthetics Carl e Misch .12Dadi SindhuNo ratings yet
- Modified Precision Lingual Bonding Technique - A Step Wise ApproachDocument5 pagesModified Precision Lingual Bonding Technique - A Step Wise ApproachUjjwal PyakurelNo ratings yet