You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Low Fat Diet PlanDocument2 pagesLow Fat Diet Planmelissa_glancNo ratings yet
- Obesity ManagementDocument24 pagesObesity ManagementAshutosh Singh100% (1)
- Canteen ManagementDocument26 pagesCanteen ManagementLeobear Corzon100% (1)
- Calculating Desirable Body Weight Using Different MethodsDocument21 pagesCalculating Desirable Body Weight Using Different MethodsWillow DumpljngNo ratings yet
- Drug Doses 2017Document127 pagesDrug Doses 2017Yuliawati HarunaNo ratings yet
- Ob GdlnsDocument262 pagesOb Gdlnsapi-3728652No ratings yet
- Jurnal Diet Keto PDFDocument8 pagesJurnal Diet Keto PDFRiza FarikaNo ratings yet
- Peter Hespel Yg IniDocument14 pagesPeter Hespel Yg IniAyi Abdul BasithNo ratings yet
- Nutrição em AtletasDocument27 pagesNutrição em AtletasSuelyne RodriguesNo ratings yet
- Comedores Tempranos Vs TardiosDocument18 pagesComedores Tempranos Vs TardiosMariana ValverdeNo ratings yet
- Analisis Upaya-Upaya Penurunan Berat Badan Pada Wanita Usia Produktif Di Wilayah Kerja Puskesmas Wawonasa Kecamatan Singkil ManadoDocument8 pagesAnalisis Upaya-Upaya Penurunan Berat Badan Pada Wanita Usia Produktif Di Wilayah Kerja Puskesmas Wawonasa Kecamatan Singkil ManadoIsnaa NurfahimahNo ratings yet
- Timing Protein Intake Increases Energy Expenditure 24 H After Resistance TrainingDocument6 pagesTiming Protein Intake Increases Energy Expenditure 24 H After Resistance TrainingAyi Abdul BasithNo ratings yet
- Growth Chart Dedi IrfanDocument40 pagesGrowth Chart Dedi IrfanAyi Abdul BasithNo ratings yet
- Vital Statistics: Measures of Disease Frequency and Mortality RatesDocument26 pagesVital Statistics: Measures of Disease Frequency and Mortality RatesAyi Abdul BasithNo ratings yet
- CH 10 Sampling Size and ErrorDocument27 pagesCH 10 Sampling Size and ErrorJajoria VkNo ratings yet
- Botulism Definition:: Clostridium Botulinum Is Found in Soil and Untreated Water Throughout The World. ItDocument3 pagesBotulism Definition:: Clostridium Botulinum Is Found in Soil and Untreated Water Throughout The World. ItAyi Abdul BasithNo ratings yet
- SurveillanceDocument21 pagesSurveillanceAyi Abdul BasithNo ratings yet
- Barriers and facilitators of weight managementDocument6 pagesBarriers and facilitators of weight managementAyi Abdul BasithNo ratings yet
- Update37 Vaccine Development PDFDocument28 pagesUpdate37 Vaccine Development PDFDevendraNo ratings yet
- Parasites in Genitourinary SystemDocument44 pagesParasites in Genitourinary SystemAyi Abdul BasithNo ratings yet
- CONCEPT OF DISEASE FayDocument39 pagesCONCEPT OF DISEASE FayAyi Abdul BasithNo ratings yet
- ANTI HYPERTENSION DRUGSDocument41 pagesANTI HYPERTENSION DRUGSAyi Abdul BasithNo ratings yet
- MICROBIOLOGY OF GENITOURINARY TRACT-2 (Julia Hartati, DR.)Document24 pagesMICROBIOLOGY OF GENITOURINARY TRACT-2 (Julia Hartati, DR.)Ayi Abdul BasithNo ratings yet
- Antiepileptic Drugs (Aed) : R. Anita. IndriyantiDocument36 pagesAntiepileptic Drugs (Aed) : R. Anita. Indriyantiandisti2323No ratings yet
- Basal Cell Carcinoma Definition:: X-RaysDocument2 pagesBasal Cell Carcinoma Definition:: X-RaysAyi Abdul BasithNo ratings yet
- Learning Objective: Lab Activity Gus Julia Hartati, DRDocument32 pagesLearning Objective: Lab Activity Gus Julia Hartati, DRAyi Abdul BasithNo ratings yet
- Parasites in Genitourinary SystemDocument44 pagesParasites in Genitourinary SystemAyi Abdul BasithNo ratings yet
- Farhan Fistel EnterokutaneusDocument34 pagesFarhan Fistel EnterokutaneusAyi Abdul BasithNo ratings yet
- Pricelist ALICA Press PDFDocument16 pagesPricelist ALICA Press PDFAyi Abdul BasithNo ratings yet
- Farhan Fistel EnterokutaneusDocument34 pagesFarhan Fistel EnterokutaneusAyi Abdul BasithNo ratings yet
- Handout 3 Activating Background Knowledge: InstructionDocument4 pagesHandout 3 Activating Background Knowledge: InstructionAyi Abdul BasithNo ratings yet
- Farhan Fistel EnterokutaneusDocument34 pagesFarhan Fistel EnterokutaneusAyi Abdul BasithNo ratings yet
- Countdown Timers For PowerPointDocument21 pagesCountdown Timers For PowerPointJeeyin MaryNo ratings yet
- WHO Europe VOL1-EngDocument70 pagesWHO Europe VOL1-EngsofiabloemNo ratings yet
- Grade 9 Weekly Home Learning Plan for October 5-9Document27 pagesGrade 9 Weekly Home Learning Plan for October 5-9Joel Nicser SingeNo ratings yet
- Malnutrition, Under Nutrition, Over NutritionDocument22 pagesMalnutrition, Under Nutrition, Over NutritionwidyaNo ratings yet
- Reading and Writing Skills LessonDocument6 pagesReading and Writing Skills Lessonkristell.dar200No ratings yet
- Progressive Resistance Exercise in The Functional Restoration of The Perineal MusclesDocument11 pagesProgressive Resistance Exercise in The Functional Restoration of The Perineal MusclesHeka Putri JayantiNo ratings yet
- The Mid Day Meal Programme of The Government of India Is Designed To Improve The Nutritional Status of School Age Children National WideDocument10 pagesThe Mid Day Meal Programme of The Government of India Is Designed To Improve The Nutritional Status of School Age Children National WideMerine JohnsonNo ratings yet
- Comorbidities and Complications of Obesity in Children and Adolescents - UpToDateDocument35 pagesComorbidities and Complications of Obesity in Children and Adolescents - UpToDatemarina alvesNo ratings yet
- Chu2018 OBESITY ImpDocument19 pagesChu2018 OBESITY ImpPoonam joshiNo ratings yet
- Format Đề Thi Không Chuyên Ptnk: Phần Trắc NghiệmDocument13 pagesFormat Đề Thi Không Chuyên Ptnk: Phần Trắc NghiệmQuảng TuyềnNo ratings yet
- 340 Windshield Survey PaperDocument7 pages340 Windshield Survey Paperapi-224141758100% (1)
- Face-to-BMI Using Computer Vision To Infer Body Mass Index On Social MediaDocument4 pagesFace-to-BMI Using Computer Vision To Infer Body Mass Index On Social MediamurakkkafsdfsNo ratings yet
- Theoretical FrameworkDocument27 pagesTheoretical Frameworkcm289867No ratings yet
- Agro NursingDocument42 pagesAgro NursingAri YuanNo ratings yet
- Topic 9 - Talking About Sports and ExerciseDocument8 pagesTopic 9 - Talking About Sports and ExerciseGénesis Pérez ThomasNo ratings yet
- Obesity TLGDocument5 pagesObesity TLGJezza Sanchez-Rellita VillariasNo ratings yet
- Management of Diabetes Mellitus XDocument182 pagesManagement of Diabetes Mellitus XPrincewill SeiyefaNo ratings yet
- J Parenter Enteral Nutr - 2013 - Choban - A S P E N Clinical GuidelinesDocument31 pagesJ Parenter Enteral Nutr - 2013 - Choban - A S P E N Clinical Guidelinescarlos enriqueNo ratings yet
- Chapter 1 SKKK4313Document89 pagesChapter 1 SKKK4313Firdaus AzizanNo ratings yet
- Health, Fitness, and Wellness Issues During AdulthoodDocument30 pagesHealth, Fitness, and Wellness Issues During AdulthoodAflaha KhanNo ratings yet
- The Triglyceride-to-HDL Cholesterol RatioDocument6 pagesThe Triglyceride-to-HDL Cholesterol RatioArthurNo ratings yet
- Apresentação de InglêsDocument2 pagesApresentação de InglêsMariana FilipeNo ratings yet
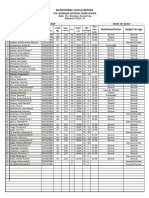
- Nutritional status report for grade 10 studentsDocument1 pageNutritional status report for grade 10 studentsdominic dalton calingNo ratings yet
- Reading Comprehension Set 1: Scientists, Chimps, ComputersDocument4 pagesReading Comprehension Set 1: Scientists, Chimps, ComputersBitan BanerjeeNo ratings yet
- Managing The Menopausal Midsection: Is It Even Possible?: Home: CorrespondenceDocument44 pagesManaging The Menopausal Midsection: Is It Even Possible?: Home: CorrespondenceArjun ShawNo ratings yet
- Emphasis of Yoga in The Management of Diabetes 2155 6156 1000613Document11 pagesEmphasis of Yoga in The Management of Diabetes 2155 6156 1000613AnuradhatagoreNo ratings yet
- Fast Food Trends in Klang ValleyDocument2 pagesFast Food Trends in Klang ValleyIda Ikhwan 이다 잌환100% (1)