You might also like
- 2 - Pressure UlcersDocument64 pages2 - Pressure Ulcerscharity kalinowsky100% (5)
- Capstone FinalDocument36 pagesCapstone Finalsamantha pabalan100% (2)
- 2022 ITECritiqueDocument80 pages2022 ITECritiqueJon LetkoNo ratings yet
- Pressure Injuries (Pressure Ulcers) and Wound Care - Practice Essentials, Background, AnatomyDocument13 pagesPressure Injuries (Pressure Ulcers) and Wound Care - Practice Essentials, Background, AnatomyKarilNo ratings yet
- Malaria: Priti Thakur Leena PestonjiDocument32 pagesMalaria: Priti Thakur Leena PestonjiPriti ThakurNo ratings yet
- WTACritical Decisions Management of Rib FracturesDocument4 pagesWTACritical Decisions Management of Rib FracturesToàn NguyễnNo ratings yet
- Pressure Ulcers and Wound CareDocument52 pagesPressure Ulcers and Wound CareKarina Mega WNo ratings yet
- Pressure UlcersDocument6 pagesPressure UlcersasuratosNo ratings yet
- NCP For FractureDocument4 pagesNCP For FracturejpNo ratings yet
- Acute Coronary Syndrome: Diagnosis and Initial Management: Each YearDocument9 pagesAcute Coronary Syndrome: Diagnosis and Initial Management: Each YearGabriela Pacheco0% (1)
- CA Coil ClipDocument12 pagesCA Coil ClipArdiansyah P PratamaNo ratings yet
- Teori Dekubitus - 1 PDFDocument9 pagesTeori Dekubitus - 1 PDFRudianto AhmadNo ratings yet
- Do All Hospitalized Patients Need Stress Ulcer ProphylaxisDocument3 pagesDo All Hospitalized Patients Need Stress Ulcer Prophylaxistsiko111No ratings yet
- Course Materials On WoundsDocument11 pagesCourse Materials On WoundsP.Senthil SelvamNo ratings yet
- Prevention and Treatment of Pressure Ulcers: What Works? What Doesn't?Document15 pagesPrevention and Treatment of Pressure Ulcers: What Works? What Doesn't?stenersonj100% (1)
- Evidence-Based Medicine: The Evaluation and Treatment of Pressure InjuriesDocument12 pagesEvidence-Based Medicine: The Evaluation and Treatment of Pressure InjuriesIndahEkaPutriNo ratings yet
- Prevention of Pressure UlcersDocument15 pagesPrevention of Pressure UlcersGabriel Urrea Botero100% (1)
- Acute Compartment Syndrome of The LegDocument2 pagesAcute Compartment Syndrome of The LegfdnjuniorNo ratings yet
- Media Fc69dcb 23Document3 pagesMedia Fc69dcb 23Ardiansyah FarizalNo ratings yet
- Pressure Ulcer Assessment and Treatment (PDFDrive)Document88 pagesPressure Ulcer Assessment and Treatment (PDFDrive)Amna AliNo ratings yet
- Critical Care For The Patient With Multiple TraumaDocument12 pagesCritical Care For The Patient With Multiple TraumaSyifa Aulia AzizNo ratings yet
- Traducir NuevooDocument21 pagesTraducir NuevooRoxana GRNo ratings yet
- Best Practices For The Prevention and Treatment of Pressure UlcersDocument15 pagesBest Practices For The Prevention and Treatment of Pressure UlcersViroj รักเมืองไทยNo ratings yet
- Prevention of Falls in Hospital: Authors: Rob MorrisDocument3 pagesPrevention of Falls in Hospital: Authors: Rob MorrisDedes SahpitraNo ratings yet
- Nursing Care ManagementDocument7 pagesNursing Care ManagementDinarkram Rabreca EculNo ratings yet
- Falls NejmDocument8 pagesFalls NejmBrijesh Jani CPC JamnagarNo ratings yet
- Prevenção QuedasDocument10 pagesPrevenção Quedasgabrielapetitot_9179No ratings yet
- The Prevention and Management of Pressure UlcerDocument5 pagesThe Prevention and Management of Pressure UlcerrantiNo ratings yet
- HSD C DandyDocument9 pagesHSD C DandyJorge MontenegroNo ratings yet
- Aafp Prevencion Caidas Tercera EdadDocument8 pagesAafp Prevencion Caidas Tercera EdadLisseth PonceNo ratings yet
- Pressure Ulcer Management in The Geriatric Patient: Geriatrics and GerontologyDocument7 pagesPressure Ulcer Management in The Geriatric Patient: Geriatrics and GerontologyKarilNo ratings yet
- 1 Bridging Anticoag Primum Non NocereDocument12 pages1 Bridging Anticoag Primum Non NocereSpencerNo ratings yet
- 0704 02 PDFDocument5 pages0704 02 PDFR4pT0r666No ratings yet
- Pi Is 0003999308015530Document19 pagesPi Is 0003999308015530Ireng PramanaNo ratings yet
- Principles of Pressure UlcerDocument13 pagesPrinciples of Pressure UlcerAmalina Elvira Anggraini100% (1)
- Johnston 2018Document23 pagesJohnston 2018cru1s3rNo ratings yet
- Lower Extremity Major and Minor Amputations in The High Risk PatientDocument6 pagesLower Extremity Major and Minor Amputations in The High Risk PatientNelson ManriqueNo ratings yet
- SVN 2023 002450.fullDocument10 pagesSVN 2023 002450.fullia_airaNo ratings yet
- The Importance of Diagnosing and Managing ICU DeliriumDocument13 pagesThe Importance of Diagnosing and Managing ICU DeliriumPablo RamirezNo ratings yet
- Pressure Injuries (Pressure Ulcers) and Wound Care: Practice EssentialsDocument66 pagesPressure Injuries (Pressure Ulcers) and Wound Care: Practice Essentialskoreta123No ratings yet
- Management of Bleeding in CancerDocument12 pagesManagement of Bleeding in CancerRoyan M. VarendraNo ratings yet
- Stroke Related Thesis TopicsDocument6 pagesStroke Related Thesis Topicskatrekahowardatlanta100% (2)
- PolipillDocument10 pagesPolipillSMIBA MedicinaNo ratings yet
- Update Managemant Unrupture Aneurysm 2018Document8 pagesUpdate Managemant Unrupture Aneurysm 2018Mikha ManurungNo ratings yet
- World Journal of Emergency Surgery: Preventable Trauma Deaths: From Panel Review To Population Based-StudiesDocument7 pagesWorld Journal of Emergency Surgery: Preventable Trauma Deaths: From Panel Review To Population Based-StudiesRita RangelNo ratings yet
- COMPASS by RISK STRATDocument10 pagesCOMPASS by RISK STRATMiguel GonzalezNo ratings yet
- Guideline For Stress Ulcer Prophylaxis in The Intensive Care UnitDocument4 pagesGuideline For Stress Ulcer Prophylaxis in The Intensive Care Unitannisa edwarNo ratings yet
- Anaesthetic Risk - HTMDocument7 pagesAnaesthetic Risk - HTMaksinuNo ratings yet
- Surgical Management of Diabetic Foot Ulcers: September 2012Document16 pagesSurgical Management of Diabetic Foot Ulcers: September 2012polin timiselaNo ratings yet
- Preventing Falls in Elderly Persons: New England Journal of Medicine May 2003Document9 pagesPreventing Falls in Elderly Persons: New England Journal of Medicine May 2003soucapazNo ratings yet
- Ma 70 379Document5 pagesMa 70 379Sonia khanNo ratings yet
- Baker Institute - No Second ChancesDocument84 pagesBaker Institute - No Second ChancesManilkkaNo ratings yet
- Why Thromboprophylaxis Fails Final VDM - 47-51Document5 pagesWhy Thromboprophylaxis Fails Final VDM - 47-51Ngô Khánh HuyềnNo ratings yet
- 1510493354article pdf1389454199Document6 pages1510493354article pdf1389454199Yolanda FitrianiNo ratings yet
- B. Caso Clinico. Turchin, I., & Barankin, B. 2006. Dermacase. Chronic Venous Insufficiency.Document3 pagesB. Caso Clinico. Turchin, I., & Barankin, B. 2006. Dermacase. Chronic Venous Insufficiency.Alex Andrés Cuevas UrriolaNo ratings yet
- The Impact of Pressure Ulcers: Bony Sacrum Coccyx Heels Hips Elbows Knees Ankles CraniumDocument48 pagesThe Impact of Pressure Ulcers: Bony Sacrum Coccyx Heels Hips Elbows Knees Ankles CraniumVanessa Camille DomingoNo ratings yet
- Rajivgandhi University of Health Sciences Bangalore, KarnatakaDocument20 pagesRajivgandhi University of Health Sciences Bangalore, Karnatakafrank.buttigiegNo ratings yet
- Clinical Notebook A Quick Mnemonic For Predicting Pressure Sores in ED PatientsDocument2 pagesClinical Notebook A Quick Mnemonic For Predicting Pressure Sores in ED PatientsChantal CarnesNo ratings yet
- Https:emedicine Medscape Com:article:2047080-PrintDocument5 pagesHttps:emedicine Medscape Com:article:2047080-Printmiss beeNo ratings yet
- DX y TX de Úlceras Venosas-2019Document8 pagesDX y TX de Úlceras Venosas-2019SaulNo ratings yet
- Varicose Veins Diagnosis and TreatmentDocument7 pagesVaricose Veins Diagnosis and Treatmenthossein kasiriNo ratings yet
- Systemic Diseases and The EyeDocument17 pagesSystemic Diseases and The Eyeapi-337689057No ratings yet
- Study of Platelet Aggregation in Subjects With Early Glucose Intolerance (EGI)Document5 pagesStudy of Platelet Aggregation in Subjects With Early Glucose Intolerance (EGI)Nestor TapiaNo ratings yet
- MastoiditisDocument3 pagesMastoiditisPrincess GyasiNo ratings yet
- Aeon Acti-PRP and A-BMC 20200908 (Fertilindo) (骨科醫美婦產泌尿)Document79 pagesAeon Acti-PRP and A-BMC 20200908 (Fertilindo) (骨科醫美婦產泌尿)RSIA Ferina SurabayaNo ratings yet
- Context ClueDocument4 pagesContext Cluemae annNo ratings yet
- Manual of Referral of Surgical Patients in Family MedicineDocument19 pagesManual of Referral of Surgical Patients in Family MedicinedrmaqsoodaliNo ratings yet
- NHSCSP 20 Colposcopy and Programme Management (3rd Edition)Document108 pagesNHSCSP 20 Colposcopy and Programme Management (3rd Edition)Sapna SNo ratings yet
- Nilai Rujukan Hematologi AnakDocument6 pagesNilai Rujukan Hematologi AnakirdinamarchsyaNo ratings yet
- NCP For HeadacheDocument1 pageNCP For HeadacheJohn MajanNo ratings yet
- Hematology: Michele L. Miller, RN, MSN-NEDocument33 pagesHematology: Michele L. Miller, RN, MSN-NEniekro35100% (1)
- Daily Regimen Ant TB TreatmentDocument37 pagesDaily Regimen Ant TB TreatmentVidya Mohan KrithikanandNo ratings yet
- 15-05-29 TBTC Soap NoteDocument2 pages15-05-29 TBTC Soap Notejhk0428No ratings yet
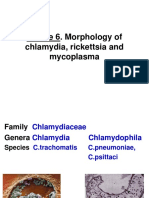
- Theme 6 ChlamydiaDocument28 pagesTheme 6 ChlamydiaAmitNo ratings yet
- Biology ThesisDocument25 pagesBiology ThesisValli RamalingamNo ratings yet
- Jurnal Urine Drainase ManagementDocument8 pagesJurnal Urine Drainase ManagementSii Silmi DestrianiNo ratings yet
- Psychosomatic Medicine 6.6.12-1Document19 pagesPsychosomatic Medicine 6.6.12-1RAHUL KUMAR DIWAKARNo ratings yet
- Thyroid Cancer Guidelines - Thyroid Nodule Evaluation, Diagnosis, Prevention of Medullary Thyroid CancerDocument10 pagesThyroid Cancer Guidelines - Thyroid Nodule Evaluation, Diagnosis, Prevention of Medullary Thyroid CancerMulyadi Abubakar BendiNo ratings yet
- PPP Reading Test 11 Part A TextsDocument4 pagesPPP Reading Test 11 Part A TextsDaniah Marwan Dawood DAWOODNo ratings yet
- Fat Embolism: Dr. Erei NunezDocument23 pagesFat Embolism: Dr. Erei NunezMan SonNo ratings yet
- E-Carts Drugs and Their UsesDocument6 pagesE-Carts Drugs and Their UsesMarienelle De La CruzNo ratings yet
- Different Types of Doctors 2022Document4 pagesDifferent Types of Doctors 2022MarcoChavezNo ratings yet
- Biomarkers For Myocarditis and Inflammatory CardiomyopathyDocument10 pagesBiomarkers For Myocarditis and Inflammatory CardiomyopathyCarlos Peña PaterninaNo ratings yet
- Cardioembolic StrokeDocument13 pagesCardioembolic StrokeFanel PutraNo ratings yet
- Alta Presyon (Hypertension)Document11 pagesAlta Presyon (Hypertension)VIERIZA MAE USMAN HAIBERNo ratings yet
- Nursing CS BurnsDocument1 pageNursing CS BurnsBai Jannah Sahida SilonganNo ratings yet
- Comparison of Rheumatoid and OsteoarthritisDocument4 pagesComparison of Rheumatoid and OsteoarthritisWaseem Khan AfridiNo ratings yet
- E Nursing LFDDocument2 pagesE Nursing LFDAlhadzra AlihNo ratings yet
- Bird Flu (Avian Influenza)Document6 pagesBird Flu (Avian Influenza)JagadeeshTJNo ratings yet